Clinical images, imperial power and Bhau Daji’s secret treatment for leprosy at the Royal College of Physicians Museum
Article DOI: https://dx.doi.org/10.15180/211501
Abstract
In 1874, Indian polymath physician Bhau Daji (1822–1874) passed away suddenly – and the details of his secretive ‘cure’ for leprosy died with him. Drawing on a collection of clinical photographs and illustrations at the Royal College of Physicians (RCP) Museum, this paper will unravel Daji’s place in the College’s empire-wide enquiry into leprosy in the mid-nineteenth century. We will argue, drawing on Elizabeth Edward’s (2014) work, that these images represent ‘photographic uncertainties’ – both conforming to and undermining traditional conventions of colonial photography, while at the same time highlighting Daji’s place as an ambiguous figure in colonial medical hierarchies. We treat the images as ‘visual arguments’ (Fox and Lawrence, 1998) testifying to the effectiveness of Daji’s secret remedy and the contagious nature of the disease. Despite the supposed objectivity of the photographic form, Daji’s treatment was never seriously investigated by the Leprosy Committee of the Royal College of Physicians. Transported from Bombay to London, we will consider the differential value placed on Daji’s medical expertise as captured by the patient images. In the spirit of the current movement to ‘decolonise collections’, we reflect on how this case study demonstrates the need for specialist medical museums to interrogate their own colonial pasts.
Keywords
Bhau Daji, collection history, decolonising, empire, leprosy, medical photography
Introduction
https://dx.doi.org/10.15180/At Dr Bhau Daji’s request, I have examined TBH aged 13. I believe I have seen this boy on a previous occasion among Dr Bhau’s leper patients while watching their treatment. At all events, I have seen photographs of young H taken from time to time… I believe the patient has been completely cured.
John Henry Sylvester, Professor of Medicine, Grant Medical College, Bombay (Boyd, 1893, p 390)
In 1893, English surgeon Stanley Boyd (1856–1916) set out to rehabilitate the reputation of Indian polymath physician Dr Bhau Daji (1822–1874) and his secret cure for leprosy. Boyd had become fascinated by reports of Daji’s mysterious remedy for this disfiguring condition – a remedy which had died with its inventor twenty years earlier in 1874 (Boyd, 1893, p 2). Reaching out across the British Empire to Daji’s former collaborators, Boyd sought to understand what lay behind this miraculous treatment, which Daji claimed could effectively cure one of the nineteenth century’s most dreaded diseases. To convince metropolitan authorities of his discovery, Daji created an archive of notes, drawings and images documenting the progress of his patients at his clinic in Bombay. Photographic evidence of the efficacy of Daji’s secret cure, as Professor Henry Sylvester, an authority at the European-style Grant Medical College, indicated in the above quote, was a central part of Daji’s approach. Yet despite his best efforts, the Daji cure for leprosy was never acknowledged in British medical circles. It was a slight that Boyd, through his extensive research, including tracking down the patient ‘TBH’, hoped to correct. He eventually conceded that the original Daji photographs, drawings and notes – and with them proof of Daji’s secret method – had been lost to history. In 2017, examples of photographs and watercolours of Daji’s patients were identified by the authors in the collections of the Royal College of Physicians (RCP) Museum in London. We believe that the RCP collection is the only surviving set of images relating to Daji’s leprosy research in Europe.[1]
To write of leprosy is to enter a long historiographical tradition of scholars who have dealt with this painful and disfiguring disease in its medical, cultural and political contexts (Bashford and Nugent, 2001; Buckingham, 2002; Anderson, 2006; Edmond, 2006; Snelders, 2017). As historian Zachary Gussow (1989) observed, leprosy is remarkable as a disease that seems to result in stigma whenever and wherever it emerges in history. However, Rod Edmond (2006) argues that responses to and understandings of the disease are unique in different periods and places. In the early nineteenth century, leprosy had largely disappeared from Europe, yet it seemed to be gaining hold in the British colonies. The imperial period of ‘lepraphobia’ was distinct from previous ages of anxiety because of its racialisation: leprosy was understood to be an illness distinctive to colonial spaces and associated with ‘unclean’, non-European colonised people (Edmond, 2006, p 7). Eighteenth-century physicians hypothesised that the disease was the result of the insidious effects of hot tropical climates acting on the perceived physical and moral weaknesses of indigenous peoples (Rush, 1799). However, the constant threat of intimate mixing between colonised and coloniser meant that leprosy came to represent ever-present ‘imperial danger’, which seemed poised to spill over into the lands of Europe (Arnold, 2017). As is often the case in this period, scientists and physicians based in the ‘metropole’ dedicated most interest to the diseases of the tropics that they deemed a threat to Europeans (Farley, 1991). By the mid-nineteenth century, attention turned sharply to the leprosy problem, culminating in an almost 40-year-long research project overseen by the illustrious Royal College of Physicians to determine whether the disease was hereditary, climate-contingent or contagious.
Photographs and drawings of leprosy patients were some of the most powerful ways that contemporary audiences in Britain came to know the dangers of the disease ‘out there’ in the British Empire. Since the 1970s, a critical scholarship has explored development of photographic technology and its use as a tool of scientific and medical knowledge-making (Gilman, 1976; Reiser, 1978; Tagg, 1988; Fox and Lawrence, 1988). With its seeming ability to create and transport ‘objective’ truths about the world, photography seemed to offer the possibility to ‘let nature speak for itself’ (Daston and Galison, 1992, p 81). From the earliest days of its invention, photography rapidly joined the ranks of other scientific tools of observation, investigation and communication, and physicians, surgeons and anatomists took up its practice with notable enthusiasm (Amirault, 1993). Indeed, the incorporation of photography into medical practice was a crucial means for the medical community to assert and consolidate authority over the body as a site of investigation (Sheehan, 2011). Photography provided a new ‘medium for seeing’ disease (Tucker, 2005, p 239), which developed into a crucial tool for diagnosis, study and communication among medical practitioners (Englemann, 2019). The creation of photographs both pictured and constructed disease by codifying its visible signs (O’Connor, 1999). Photographs, like field notes, instruments and maps, were part of an arsenal of technologies and strategies, labelled by Bruno Latour (1987) ‘immutable mobiles’, which aimed to assist supposedly objective scientific facts to transcend spatial contexts (Livingstone, 2003).
In the colonial context, scholars have observed how anthropological and medical photography served to create and reinforce hierarchies of power and racial difference. Images of ‘othered’ colonial bodies, ‘used to frame the character and physiology of the colonized as a series of ranked types’, were a crucial way in which domestic audiences were taught to know (and feel superior to) ‘their’ empire and its peoples (Peffer, 2009, p 242; Bennett, 1995; Stepan, 2001; Qureshi, 2011; Roque and Wagner, 2012). Photography in colonial settings is often seen as an element of a broader group of visual technologies and practices developed to support imperial governance and to exert control over indigenous bodies, including anthropometry, tattooing and fingerprinting (Sengoopta, 2003; Anderson, 2004; Waits, 2016). As Elizabeth Edwards (cited in Peffer, 2009, p 242) has observed in her numerous studies of anthropological photographic practices, photographs of indigenous peoples ‘served both to symbolise the power differential in the colonies, and to bring it into visible order’.
Most scholarship on photography in colonial settings has been predicated on a colonised-coloniser relationship in which ‘highly conspicuous’ imperial servants photographed suspicious, resistant or docile ‘natives’ (Ryan, 1997, p 144). Yet a growing literature of colonialism and resistance urges us to think in more nuanced ways about what many scholars argue has been an overly binary understanding of the colonised-coloniser relationship (Schaffer, Lissa, Kapil and James, 2009; Johnson and Khalid, 2011; Chaudhary, 2012; Wagner and Roque, 2012; Domingo, Jerónimo and Roque, 2019). Undoubtedly, much photography in colonial settings was characterised by coercion and even violence, as the photographed had little or no control over the ways in which their bodies were appropriated for the camera (Vokes, 2018). However, class, gender, race, differential structures of power, influence and mobility complicate the encounter between people in a colonial setting. Photographs of colonial people as cultural artefacts, whether medical, anthropological or otherwise, represent a form of colonial knowledge, an ‘expression of worlds and visions brought into contact’ (Wagner and Roque, 2012, p 4). New work in colonial photography has not moved to negate the observations of earlier studies but serve to provide more nuance (Geary, 2003; Buckley, 2010; Vokes, 2018). The Bhau Daji collection of photographs and watercolours offers an insightful case study in the multivalent aspects of colonial medical photography. European control of the camera was far from total. In this group of images, an Indian physician photographed his patients of many ethnic backgrounds. Deeply complex images, they bring into question assumptions about the racialisation of disease and medical authority. In this paper, we will consider how these images represent a dual colonial action – at once opening up anxieties about the transmissibility of leprosy to white European colonists while also revealing the colonial hierarchies of power in the translation of Daji’s medical expertise from a colonial space to a metropolitan setting.
Daji himself is a significant figure in the history of medicine in India. A Sanskrit scholar well versed in the ancient medical and philosophical traditions of India, he was also a paragon of a new, ambitious class of Indian intellectuals, trained in European medicine at institutions like Grant Medical College. An ‘intermediary’ figure, Daji at once reinforced typical metropolitan conventions of medical science, while integrating indigenous forms of knowledge (Johnson and Khalid, 2011).

In this light, this paper will suggest that the Daji images may be understood as ‘photographic uncertainties’ of empire as conceptualised by Elizabeth Edwards (2014). Such photographs, Edwards argues (2014, p 173), should not be viewed as simple instruments of empire, but instead as ‘ambiguous and indeterminate modalities of colonial governments’, which can have multiple and overlaid meanings. She encourages historians to closely consider individual images and to tease out the assumptions, expectations and potential uses which they embody. We suggest that the Daji images represent their maker’s attempt to legitimise and convince metropolitan authorities of his medical expertise and the effectiveness of his cure. However, how Daji intended them to be viewed and how they were received by the Royal College of Physicians were quite different. The images are ‘ambiguous’ – at the centre of many lookings and seeings which varied with geographical and institutional context, an analysis of which serves to illuminate questions of medical authority in a trans-imperial light.
The Royal College of Physicians may seem an unusual location in which to encounter these imperial artefacts. Founded in 1518, the College’s central purpose was to regulate the medical profession in London and its surroundings – meting out justice to irregular practitioners who did not (or were not permitted to) gain its license. Today, the College’s museum is best known for its extensive collection of portraiture showing Members and Fellows, and for its ceremonial silver (Jordanova, 2018). Notably, the institution’s portrait collection is overwhelmingly white and male – a fact brought starkly into light in 2018 with the College’s ‘Women in medicine’ exhibition and the acquisition of the institution’s first portrait of a non-white sitter into the collection that same year (Hussey, 2018). As historians of medicine and empire have observed, the imperial contexts of British medicine are often overlooked (Haynes, 2001; Chakrabarti, 2014; Hussey, 2021), with some historians like Niall Ferguson (2011) continuing to insist that the importation of western medical practices to colonial spaces was a ‘benefit’ of the imperial project.
This paper will demonstrate that despite the Eurocentric impression given by its exhibitions, the College has deep, historic entanglements with empire through its research into leprosy. In the tradition of post-colonial scholars like Antoinette Burton (1994, 1998) and Catherine Hall (2002), we view colonial and metropolitan spaces as mutually constitutive, and approach the RCP as a locus of knowledge making whose networks spanned British and colonial places, people and things. Like Bruno Latour’s (1987) ‘centre of calculation’, the London-based RCP purposefully fulfilled a role as arbitrator of authoritative medical knowledge both at home in Britain and in the empire. As a result, a close analysis of the Daji photographs can reveal more not only about Daji’s life and research, but the ways in which leprosy as a disease category and photography as a tool of authority were created within imperial power structures that spanned the ‘imperial social formation’ (Sinha, 1995, p 2). We will suggest that it is through such critical collections research that small, specialist museums like the RCP can come to acknowledge their colonial pasts and decolonise their collections.
The Bhau Daji method
https://dx.doi.org/10.15180/211501/002Bhau Daji (or Bhow Dajji) was an important figure in mid-nineteenth century Indian medicine and a prominent antiquarian. Born Ramkrishna Lad in 1822, he grew up in Goa with his father, Vithal, and his younger brother, Narayan. Ten years later, Vithal moved his family to Bombay, where Daji’s reputation as a prodigy still endures (Mukhopadhyay, 2018, p 114). According to his biographers, he was an avid chess player by the age of ten and his capacity for brilliant strategic thinking well beyond his years caught the eye of the Governor of Bombay. The Governor was so impressed that he encouraged Daji’s father to give his son the best education possible and the young Daji went on to attend the prestigious Elphinstone College in 1840 (Keer, 1963; Mainkar, Bhandarkar and Dar, 1974; Naik, 1995; Mukhopadhyay, 2018). It was there that he developed an interest in social, educational and political reform – advocating against female infanticide, supporting the education of women, and campaigning for widow remarriage (Mukhopadhyay, 2018, p 115). Daji was among the first students to train as a physician at the newly established Grant Medical College in Bombay – one of the first European medical schools founded for the training of Indian practitioners.

By the middle of the nineteenth century, European physicians had been practising medicine in India for nearly 300 years. However, these physicians had focused almost exclusively on the treatment of other Europeans, and the care of colonised peoples was mostly left to practitioners of indigenous medical systems. With the increasing formalisation of British control over India, so too did European physicians seek to establish their dominance over medical practice in the Raj. Western-style medical schools like Grant Medical College sought to do away with, in the words of Charles Morehead (1807–1882), ‘the demoralising effects of the irrational, superstitious, and, too often, criminal empiricism’ of native doctors through the education of Indian practitioners (quoted in Pandya, 2004, p 295). Shubada Pandya (2004, p 296) has argued that training at an elite college like Grant helped to establish an influential and powerful new class of Indian private practitioners – who went on to challenge the supremacy of the British dominated Indian Medical Service. Daji was one of only three Hindu students in the inaugural class, largely due to religious prohibitions around the dissection of human bodies. Nevertheless, Daji excelled at Grant, graduating in 1851 and opening a dispensary with his brother (Ramanna, 2000, pp 51–52). In this same period, he also became a respected Sanskrit scholar. He published several articles in Bombay’s Royal Asiatic Society Journal and he was known for his interest in and ability to interpret the ancient Elephanta inscriptions. Daji played a role in the creation of the Victoria and Albert Museum, Bombay (now the Dr. Bhau Daji Lad Museum, Mumbai) and was a founding member of the Photographic Society of Bombay. His brother Narayan was a talented photographer in his own right, with his work being exhibited at early Society meetings (Pinney, 2008, pp 12–14).
In the late 1850s, Daji became engrossed in researching and finding a cure for leprosy (Boyd, 1893, p 389). Contrary to European theory, Indian physicians believed leprosy to be contagious and curable. As a student of both eastern and western education with an extensive knowledge of Sanskrit texts, Daji was in a unique position to blend both knowledge systems. The Ayurvedic tradition had a well-established set of therapeutic practices for the disease, which had been plaguing the Indian subcontinent for centuries. Daji continued to work throughout the 1860s on his cure by studying the relief-bringing remedies of indigenous communities through a western approach of experimental investigation. Not long after, Indian newspapers began publishing letters from his patients detailing their experiences of his treatment, which caught the attention of the medical press in Britain (Boyd, 1893, p 389). Despite these glowing testimonials, The Lancet (‘The cure of leprosy’, 1868, p 238) expressed their scepticism at Daji’s methods, writing:
The statements that have now been made as regards better success are necessarily received by us with suspicion. Dr Bhau Daji’s first step should be to make known his remedies and his mode of procedure. Opportunities for putting them to the test will occur in England.
Daji’s insistence on keeping his remedy secret ruffled feathers both in India and in Britain as it contravened the ‘rational empiricism’ on which western medical practice prided itself (Pandya, 2004, p 305). Ironically, it was due to this metropolitan scepticism that Daji resolved to keep his remedy a secret until all of his trials and investigations had been thoroughly analysed. As he remarked:
Knowing the numerous fallacies that are liable to influence inferences drawn from observations imperfect in themselves, or few in number, I am collecting for the Profession…data on a large scale (comprising three or four hundred cases) from which to make deductions with regard to cure, conditions of treatment (quoted in Pandya, 2009, p 98).
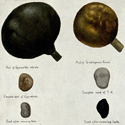
Unfortunately, Daji’s ambitious project was interrupted by his sudden death. What we know today of the Daji method is the result of English surgeon Stanley Boyd’s later research into his work. Boyd discovered that at the time of Daji’s death, even Narayan did not know the secret behind the cure. His greatest breakthrough in unravelling the mystery was identifying and interviewing the father of a former patient – a young male European known as TBH, who had left India after this treatment and was now living in London and working as a carpenter. Given the stigma attached to the disease, the man would not reveal his son’s name and was reticent to share many details. He reported that he had destroyed the photographs of his son with the disease and had managed to keep his former condition a secret even within his family. Reviewing the evidence, Boyd came to the conclusion that the Daji method relied mainly on the topical and internal application of chaulmoogra oil (Hydnocarpus wightianus), along with a strict vegetarian diet, although the complete treatment regimen remained a mystery.
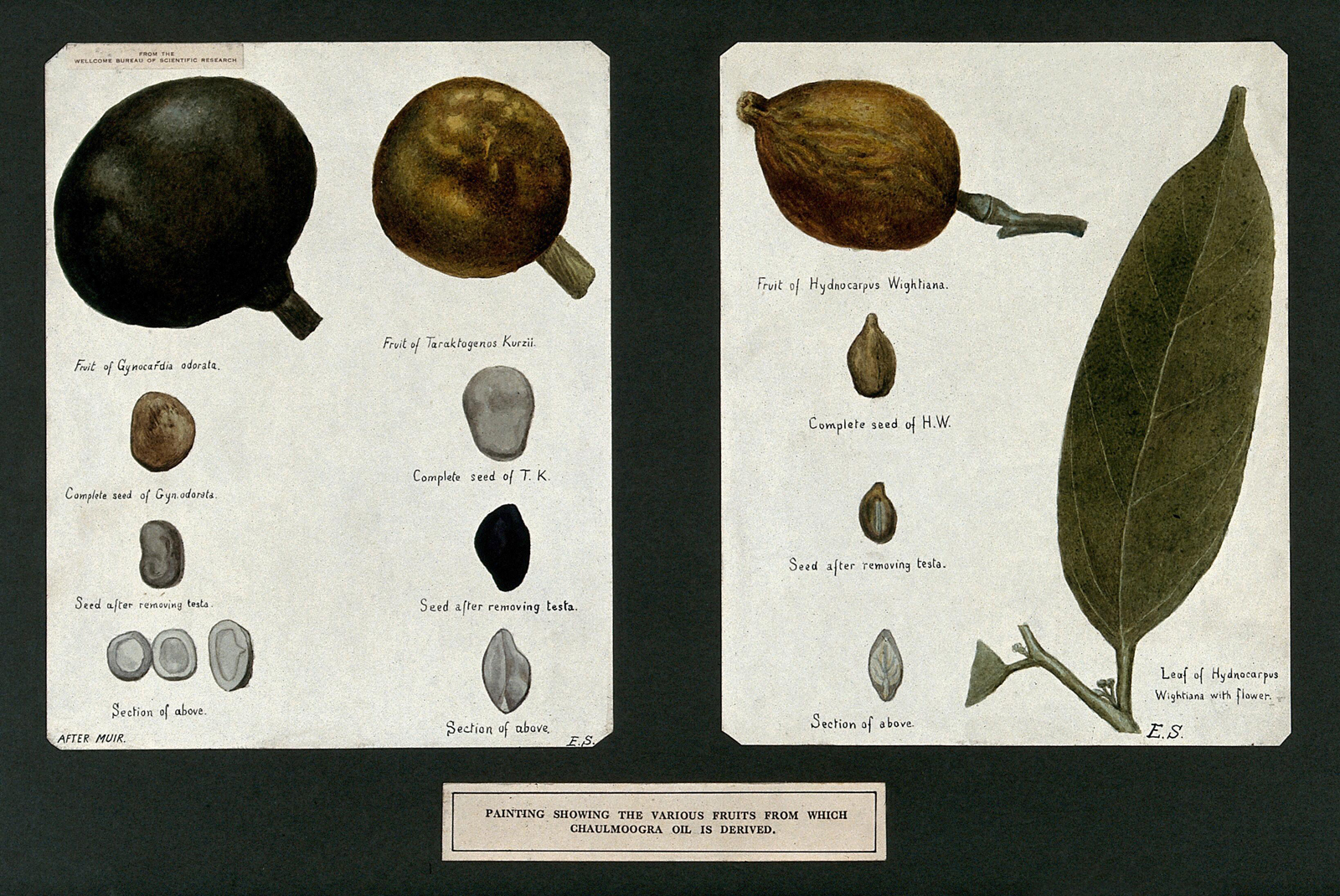
While chaulmoogra oil was not widely used in Europe until the early twentieth century, in India its use to treat leprosy and other dermatological diseases stretches back over two thousand years. The Sushruta Samhita, one of the foundational ancient Sanskrit texts on medicine and surgery, describes both the clinical features and treatment of leprosy around 600 BCE (Dharmendra, 1947, pp 424–430). Employing his extensive knowledge of Indian history and remedies Daji was uniquely placed as an interface between indigenous knowledge of plant medicines and European approaches to disease. Despite Boyd’s efforts, however, Daji’s name failed to be associated with the use of chaulmoogra oil in the treatment of leprosy. Nevertheless, the oil entered into widespread use in colonial medicine in the early twentieth century – publications such as The Lancet reported on the many cases in which injectable and topical treatments were becoming more and more commonplace (Rogers, 1921). Daji’s remedy continued without him well into the first half of the twentieth century and stood as the preferred method of symptom relief until the 1940s when sulfonyl antibiotics were introduced (Parascandola, 2003, p 48).
Picturing leprosy
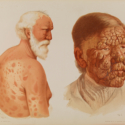
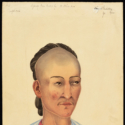
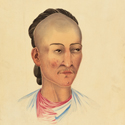
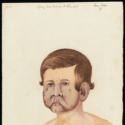
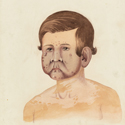
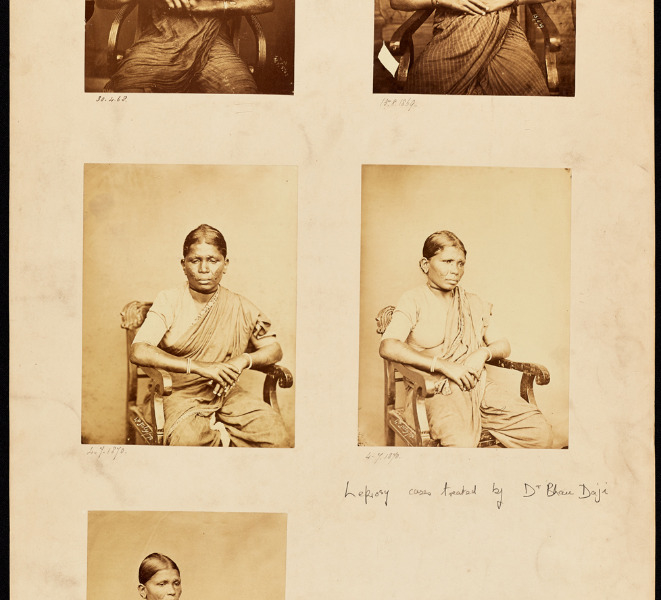
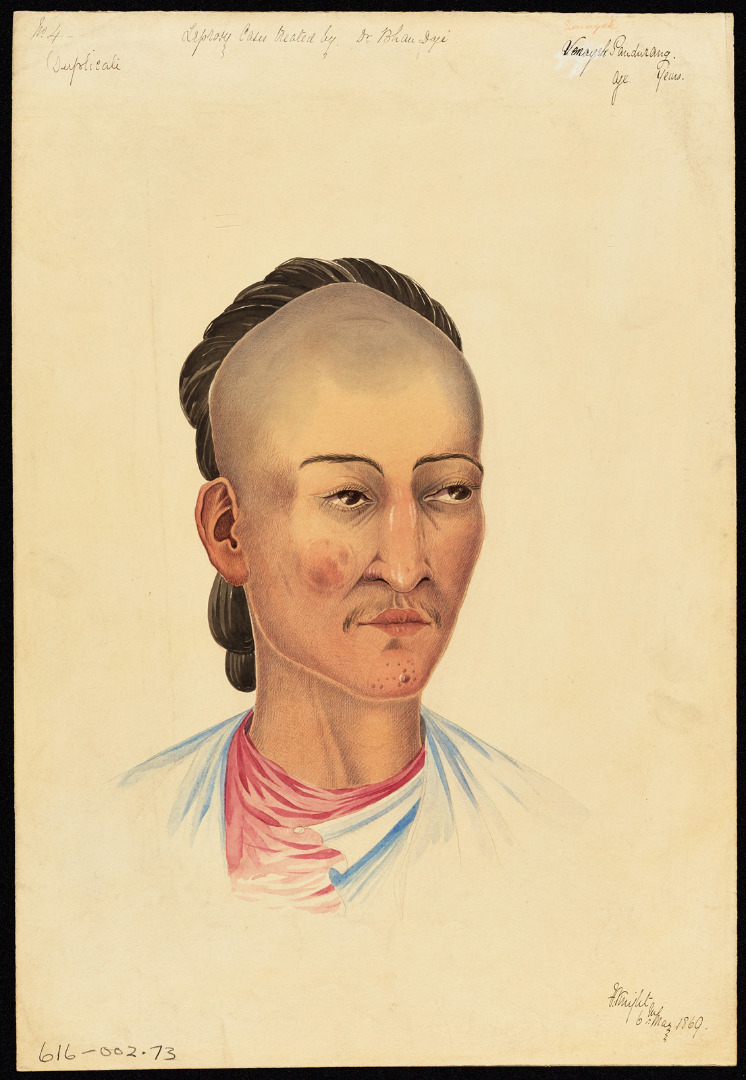
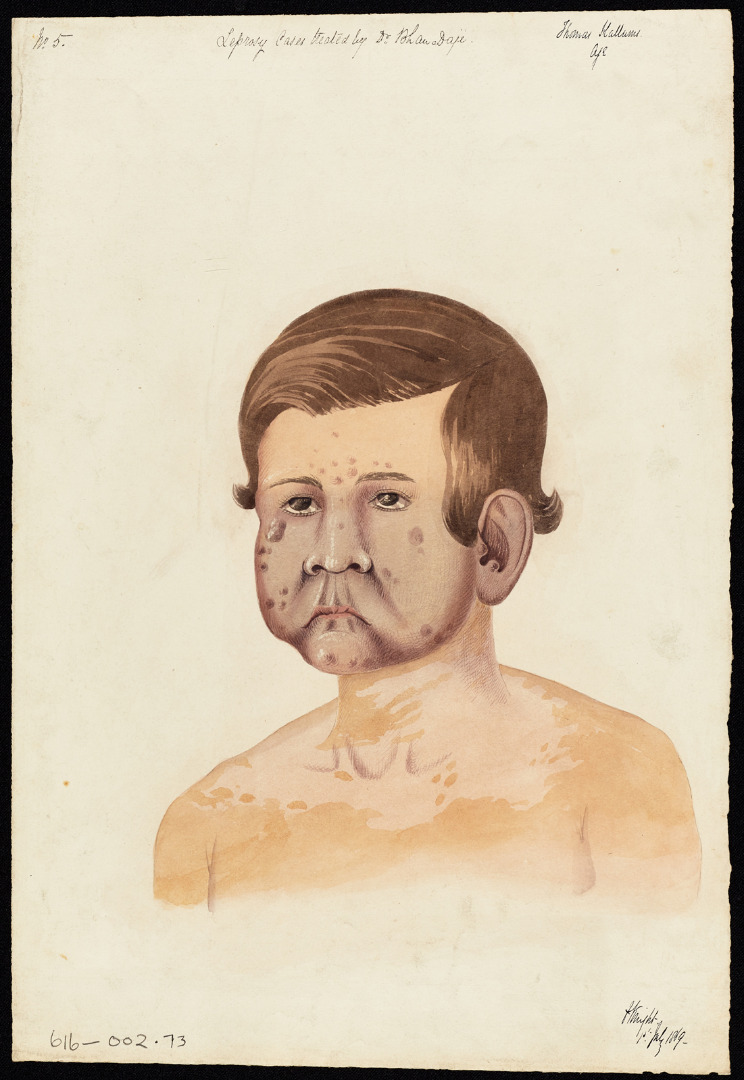
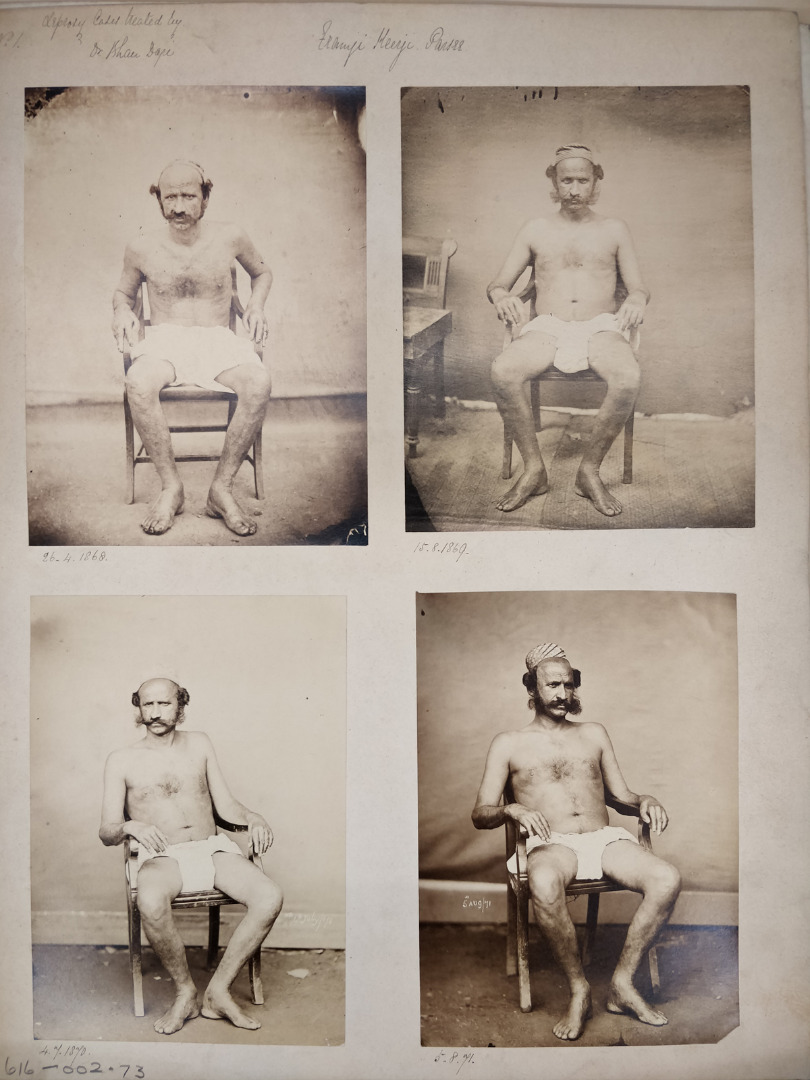
https://dx.doi.org/10.15180/211501/003The Bhau Daji collection at the RCP consists of 12 items: eight sheets of clinical photographs showing numerous images of six named individuals, accompanied by four watercolours.[2] They are all labelled with the title ‘Leprosy cases treated by Bhau Daji’, followed by the name and ethnic origin of the patient shown, as well as dates. The names of the patients are given as Daddaje Narayrn, a ‘Hindoo’, Franji Heerji, a ‘Parsee’, Thomas Hallums, a ‘European’, Esseera Cassia Settia, a ‘Hindoo’, and a Hindu woman named Gunga Babbaji. The watercolour portraits show detailed views of the faces of Hallums, Babbaji, Settia and an additional patient named Venayak Pandurang, who does not appear in the images (or of whom the photographs have been lost). The watercolours are credited to the artist F Knight, but the name of the photographer is not stated. However, the images may well have been taken by one of the Daji brothers, given their keen interest in photography (Hapgood, 2015). As the photographs have been glued to the pages, it is not possible to ascertain whether further information is written on the reverse. The images show the patients in various stages of healing, dating between April 1868 and August 1871.[3]
Like the photographs used for recording ‘racial types’ in anthropology, medical photography in colonial sites was inexorably bound up in perceived hierarchies of race, and diseases as manifestations of the supposed subordinance of colonised peoples (Gilman, 1995; Stepan, 2001; Edwards, 2014). Sadiah Qureshi (2011) has argued that colonial photographic practices served to reinforce the dichotomy between white viewer and black subject. These model the power dynamics of western photography in the colonies; underlined by a tacit understanding that such images represent a white expert photographing a colonial subject, typically a person of colour. However, in these images we have Daji, an Indian physician, photographing people of many different ethnic origins, including a European patient. These images require a more nuanced reflection of the many different kinds of colonial encounters behind the production of medical photography. What were the material contexts of their production, the nature of the documentary impulse which motivated Daji, and the potential experiences of the sitters, his patients? By reading the photographs not as ‘facts’ but as a ‘visual argument’ (Fox and Lawrence, 1998, p 7), conceived by the physician Daji, we can gain greater insight into the practice of colonial medial photography and the ways in which it was here used to represent Daji’s research and therapeutic practice. The photographs are ‘uncertainties’ which at once reinforce standard conventions of colonial medical photography, while undermining colonial hierarchies of seeing.
Scholars have observed that physicians made use of photography for the purposes of documentation almost as soon as the technology was made widely available in the 1840s (Hattori, 2011). As Tanya Sheehan (2011) has observed, it is difficult to disentangle the medical elements from the conventions of early photography. Indeed, she suggests that the ‘mutually constructive’ relationship between commercial photography and medicine saw photographers and physicians using each other to secure their authority (Sheehan, 2011, p 7). Early clinical photographs aimed to show the patient and to capture and codify the visual features of their disease – often in poses which served to draw the viewer’s eye to the affected body parts. While by the 1890s clinical photography had acquired many of its own conventions, in the 1860s and 70s medical photography followed many of the same norms as portrait photography (Fox and Lawrence, 1988; Amirault, 1993). However, it should be recalled that unlike studio photography, clinical photographs were often painful and exposing to take, the individual’s diseased body or body parts subsuming their individual identity. In Erin O’Connor’s words, ‘Half artistic interpretation, half documentary device, medical portraiture operated to bring out the individuality not of the sitter, but of the sitter’s disease’ (1999, p 235). In both colonial and ‘western’ contexts, medical photographs represent a sensitive encounter, in which a patient’s sense of self and bodily autonomy were challenged to produce images for which they had little or no control over their subsequent use.
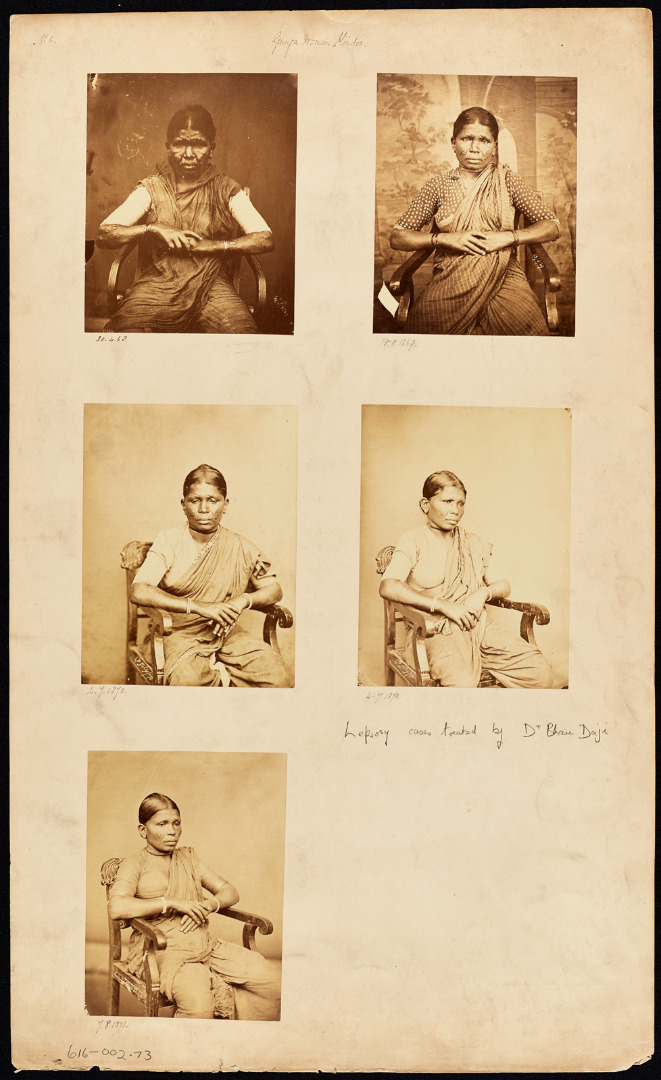
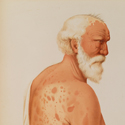
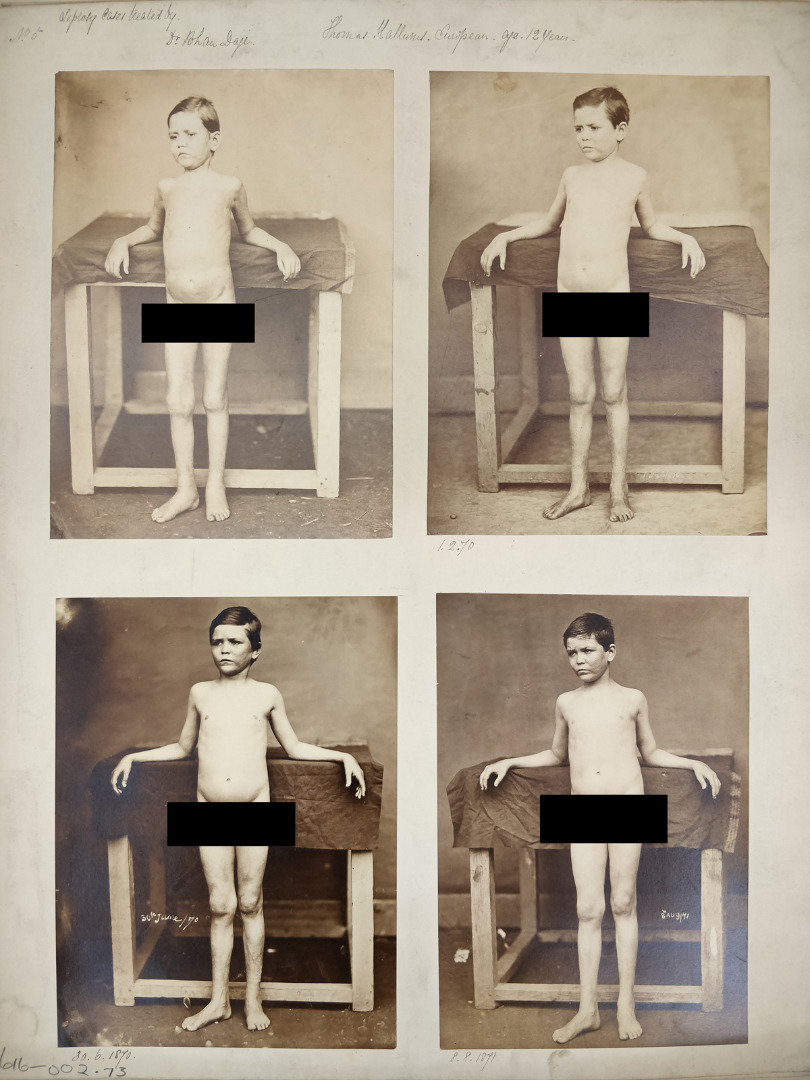
In the Daji images, the patients are carefully posed, often in front of decorative backdrops and in very deliberate positions. As with most clinical photography, the emphasis is on the image capturing the diseased body rather than the individual, leading to the erasure of individual agency and identity. Like with anthropological photography in which the sitter comes to stand in for a ‘type’, in medical photographs the person becomes their disease – or in the case of Daji, a visual manifestation of treatment. The subjects are seated or posed on chairs and other props which allow them to show to advantage the diseased parts of their bodies. In order to facilitate this emphasis on the signs of leprosy patients are in various states of undress, ranging from Hallums, shown completely nude, to Babbaji, who remained completely clothed.
Undoubtedly exposing and uncomfortable, nudity was a common feature in both colonial medical and anthropological photography, as well as clinical photography in Europe and America of this period – allowing the photographer to show the physiognomy of the body or signs of disease to the viewer (Ryan, 1997). It is not clear whether these photos were taken in a photographic studio or whether props and backdrops were brought to Daji’s clinic, although the latter arrangement is more likely. While European authorities were not convinced of the contagious nature of leprosy, in the Indian context it was widely believed the disease could be spread through contact. It must also be remembered that sufferers of leprosy were heavily stigmatised, and the patients pictured likely would not have wanted their status as lepers to be known in the community.
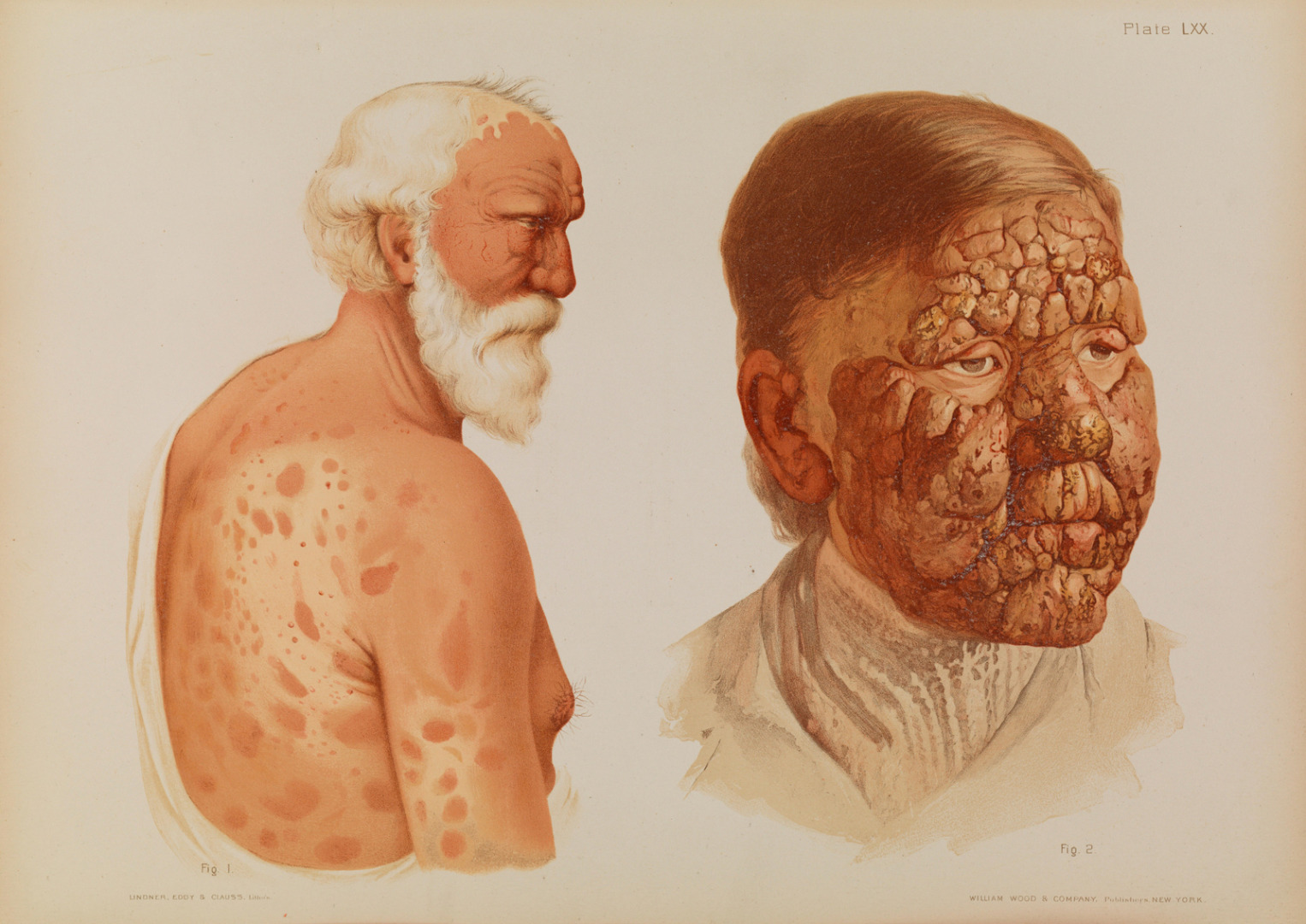
Photography was especially well suited to capturing ‘pathology as surface’ – and diseases that affected the skin (like leprosy) were particularly well suited to this approach (O’Connor, 1999, p 234). However, it is informative that some of the photographs are complemented by watercolour portraits. As scholars of photographs have observed, the quality of photographs in this period made them in some ways a poorer alternative to the supposedly more subjective medium of watercolour or painting (Edwards, 2014, p 172). The black and white, often washed out nature of early photography made it difficult for viewers to see the details, which were especially important when the subject of the image was medical (Fox and Lawrence, 1988, p 22). The watercolours therefore serve to reinforce the images – providing greater detail on the colour and texture of leprotic lesions to enhance or verify the truthfulness of the photographs. As Edmond (2006, pp 9–10) has argued, the dark colour of leprosy lesions raised the spectre of racial degeneration – with leprosy seemingly transforming ‘civilised’ white bodies into colonised ‘black’ ones. Black and white photographs would not have been able to capture the subtle physical changes which made this disease so terrifying to white colonists.
What exactly were contemporary viewers intended to understand from these photographs? The serial nature of the images showing the same patient over time suggest that they are intended to convince the viewer of the efficacy of Daji’s cure. For example, Heerji’s photos demonstrate how careful attention was paid to reconstructing the exact same pose with similar clothing over several years as a way to draw the viewer’s eye to subtle changes in the visible body and skin. In the first image, the patient seems thin and worn out; the uneven tone and texture of the skin attests to the presence of leprosy. By the final image, the patient has gained weight, his face is more composed, he sits at ease in his chair and his legs and arms look noticeably smoother.
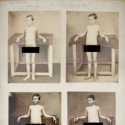
A similar progression can be viewed in Hallum’s case. In each photo, the boy is propped up against a stand which facilitates the opening of his arms and chest – the same pose repeated over several years. The viewer would see the boy not only age but also gain weight and a noticeable change occur in the texture of his facial skin and that of his arms (see Figure 7). To a medical viewer aware of the seemingly unstoppable degenerative progression of leprosy, such changes shown over time would have been viewed as remarkable. Almost certainly this image shows TBH – the young patient whose progress so astounded Professor Sylvester and who Stanley Boyd was able to track down in his retroactive research into the Daji method. It is a rare occurrence, as researchers, to be able to re-unite clinical histories with images of individual patients – particularly in Hallum’s case, where his diagnosis was a closely guarded family secret. Of all of the images taken by Daji, Hallum’s was likely to be of the greatest interest to metropolitan audiences as it visually demonstrated the manifestations of a supposedly ‘native’ disease in a European child.
The poses, setting and props mark these images as typical of medical photography of this period, regardless of geographical boundaries. Yet we know that the photographs differ in one crucial way – they have been composed by Daji himself. Trained by prominent physicians in a European medical school, we would like to suggest that Daji used the conventions of British medical photography as a mechanism for convincing European eyes of his cure. To achieve this aim, it was undoubtedly necessary that he conform to the ‘correct’ modalities of western clinical photography as closely as possible. The relative state of undress of the patients, the poses in chairs, or with bodies turned front and back, closely resemble racial photography of the period (Ryan, 1997). Yet some differences are worth remarking upon. Firstly, the only patient to be depicted completely nude is the European one – the other patients are permitted to retain at least some items of clothing, at a minimum to cover their genital area. This is possibly because in Hallums’ case, Daji is attempting to show healing is occurring in the lower abdominal region, which may have been unhelpfully covered by Hallum’s usual clothing (see Figure 7). Secondly, the only female patient, Babbaji, is allowed to remain completely clothed. While it is of course possible that her leprotic lesions were confined solely to the face and forearms, it is our belief that this choice was more likely one made to respect her wishes and the conventions of modesty (see Figure 6). One could argue that his relationship with his female patients was feasibly informed by their embeddedness in the local context – resulting in a mutual respect of modesty practices often pushed aside by European medical practitioners. Speculatively, we may conclude that Daji’s place in colonial racial hierarchies has informed the images produced – one in which colonised bodies are allocated a greater respect and European ones more exposed.
The College and the Leprosy Committee
https://dx.doi.org/10.15180/211501/004It may be at first puzzling to think that these complex and nuanced images of leprosy in the British Raj found their way into the Royal College of Physicians of London. An august institution founded by King Henry VIII, the College tends to appear in histories of British medicine as a protectionist bastion of privilege – an organisation most interested in guarding the esteem and careers of its few elected Fellows (Brown, 2011). In the nineteenth century, the College leadership was increasingly under pressure to reform its structures, which were perceived as overly London-centric. Indeed, some scholars have argued that colonial medical practice served as an ‘escape valve’ for new entrants into the profession who found their way blocked by the restrictive grip of College members and Fellows on the best positions in the capital (Harrison, 1994; Haynes, 2006). Nevertheless, the College was involved in a number of less remarked upon initiatives of broader geographical interest across the nineteenth century – its survey of imperial hospitals, for example, and its role in advising the British government on cholera responses and its leprosy survey (Cooke, 1972). In attempting to answer pressing questions about the nature of leprosy (its pervasiveness, its contagiousness), the College accumulated what Bruno Latour (1987, p 223) has characterised as ‘immutable and combinable mobiles of knowledge’ – questionnaires, statistics and photographs which served as the material proof necessary for creating new and authoritative knowledge of the disease. As a ‘centre of calculation’, the College exerted a strong pull on ‘immutable mobiles’ such as the Daji photographs – drawing them across imperial spaces.
In May of 1862, the Secretary of State for the Colonies forwarded to the College a letter from the Governor of the Windward Islands in Barbados who was concerned by what he saw as the ‘increase’ of the ‘fearful malady’ of leprosy in his colony (quoted in Milroy, 1867, p 2). The College leadership decided that it would wade into this issue, undertaking to ‘collate, digest and report upon whatever information respecting the disease of leprosy in the Islands under Governor Walker’s government or elsewhere’ (Milroy, 1867, p 2). In the end, an interrogatory was circulated not just to the West Indies but across the British Empire in India, China and the South Pacific. It was a bold suggestion and a massive undertaking for the College – one that would occupy its Leprosy Committee for the remainder of the century. The College received hundreds of responses from medical men, colonial administrators, missionaries and other respondents across the globe in response to their 17-question survey. Respondents were invited to answer the questions as well as submitting other supporting documents like ‘reports of post-mortem examinations or any pictorial illustrations’ (Milroy, 1867, p lvii). These responses were then collated by the specially appointed Leprosy Committee, led by Edinburgh-trained epidemiologist and physician Gavin Milroy (1805–1886), and finally published in a report in 1867.
While the College was interested in obtaining information about the disease generally, they were specifically interested in ascertaining whether leprosy was infectious or not. It was a question with far-reaching consequences for colonial governments – who would be forced to enact expensive and disruptive quarantine policies should it prove to pass person-to-person. For most practitioners it was difficult to distinguish leprosy from other dermatological and tropical diseases like syphilis, scrofula, yaws or elephantiasis. It was variously thought to be sexually transmitted or possibly directly contagious, maybe caused by the consumption of breadfruit or, for famous physician Jonathan Hutchinson (1879; 1906), caused by eating salted fish. As Gerard Hansen, the Norwegian physician who later discovered the bacteria which cause leprosy, stated, ‘There is hardly anything on Earth, or between it and heaven, which has not been regarded as the cause of leprosy’ (quoted in Manson, 1906, p 508). Ultimately, the College report came down on the side of the hereditary nature of leprosy – arguing in contradiction to a contemporary controlled study by Daniel Danielssen and Carl Boeck (1848), who demonstrated its contagiousness. Indeed, the College continued to insist that leprosy was not contagious almost into the new century, only relenting when the first International Leprosy Conference held in 1897 made their old-fashioned stance seem almost ridiculous.[4]
While the 1860s saw the beginning of a general turn towards specific causes of disease, the College Fellows held fast to a long tradition of environmental medicine, which saw disease as the result of environmental factors like miasma. As a result, they were suspicious of reports of leprosy ‘cures’ that fundamentally contradicted this firmly held stance. Yet only a year after the publication of the committee’s first official report, the medical community was sent aflutter by reports of a miraculous cure for the diseases being trialled by Dr L D Beauperthuy, a French physician working in Venezuela (Darwin, 1871, p 434). The College received information on the success of the ‘Beauperthuy’ method through an intermediary named Robert Bakewell – a Manchester-born surgeon who had moved to Trinidad to undertake a post as Vaccinator General (Edmond, 2006, p 87). Milroy was naturally suspicious as he retained his strongly held belief that the disease was hereditary. However, Bakewell’s reports were convincing enough that Milroy himself travelled to South America to view the results in person. That the College felt they needed a representative to see the facts with their own eyes is revealing of the frustrations they had previously faced in ‘knowing’ leprosy at a distance. In his published report in 1873, Milroy debunked the Beauperthuy method – but saw some usefulness in an adaptation of it using cashew nut oil, which seemed to provide some symptomatic relief from the disease.
It was during this tumultuous period that the Daji photographs and watercolours arrived at the College in London. In the move from Daji’s ‘on the ground practice’ in Bombay to the far-removed ‘centre of calculation’ represented by the RCP, the perception of the images underwent a profound change. For Daji, they may have been representations of the efficacy of this work and (possibly) the sensitivities of the doctor-patient relationship amongst a broad clientele that spanned different ethnic and class groups. However, in this new context of the RCP’s quest to ‘know’ leprosy, situated at the crossroads of their imperial networks of informants, we must attune ourselves to their differential value. Here the question becomes not only the extent to which leprosy is curable, but which technologies of testimony and which speakers of this testimony were reliable sources at a distance. As Wagner and Roque (2012, p 13) observe, ‘the emergence and categorization of “colonial knowledge” as credible or trustworthy is an unstable, tensional, and contingent event’ – reflective of technological, material and spatial contexts, and the interests, desires and tensions amongst actors and institutions. As ideas circulate, they are not merely migrated but translated – subjected to new regimes of power and perception as they move between spaces.
It is recorded in the College’s Annals that on 26 January 1872, George Campbell, Secretary of State for India (and later Duke of Argyll), sent to the College a collection of ‘photographs and coloured drawings by Dr Bhow Dajii of Bombay in Connection with a cure for leprosy which that gentlemen trusts he has discovered’.[5] Campbell was politely thanked for his gift, and the photographs, as well as Bhau Daji, are not mentioned again in the records of the College meetings. This perfunctory response is notably different from the outpouring of extraordinary meetings held to discuss the Beauperthuy method and the in-depth discussions of various other communications about leprosy and purported cures in this period. There could be many reasons for this marked lack of interest in the photographs – perhaps the intellectual (and financial) resources of the College had already been exhausted by the extensive investigation into Beauperthuy’s claims. Perhaps the committee members felt the photographs did not show enough new or compelling information to merit further discussion. However, it is our contention that the committee’s apathy was not due to the potential persuasiveness of the photographs as an evidential tool but rather in the lack of metropolitan authority granted to the Indian practitioner whose research they intended to demonstrate.
Our reasoning for this interpretation is twofold. First, we know from discussions of the materials received as a part of the original leprosy survey that the College placed a great importance on photography as evidential material. Despite having explicitly asked for photographs of patients, in the final report Milroy bemoaned the lack of pictorial representations the Leprosy Committee received. The Lancet in its review of the report was especially disappointed by the lack of information on specific cases – whether case notes or post-mortem reports (‘Editorial: The Leprosy Report of the College of Physicians’, 1867, p 64). Even amongst the small number of photographs that were sent from Bombay, Ceylon and Hong Kong, the College reviewers declared themselves unimpressed with clinical images which did not track specific individual’s treatment over periods of time, and were especially critical when dates, names and ages were not provided.[6] ‘Citations of the mere opinions of various writers…are of little avail in determining a question of facts.’[7] In their emphasis on the fact that images were not on their own ‘factual’ unless accompanied by specific additional contextualising information, the College authorities mirrored wider trends in science that aimed to render photography more accurate and reliable. For example, the shift towards anthropometrics as a way of creating pure ‘mathematically legible documents’ (Edwards, 2016, p 92). Yet the Daji photos abide by all these conventions of ‘convincing’ clinical photography – showing patients progressing over several years, with names, dates and details all carefully annotated. They are, in short, exactly the sort of visual, factual evidence on leprosy that the College was seeking. Nevertheless, the photographs were not afforded a level of interest expected of supposedly objective and compelling scientific artefacts.
Secondly, an argument for growing disinterest in the topic does not match the level of discussion and research which leprosy and its potential cures received in College meetings and publications in this period. The Beauperthuy affair was far from the last large-scale effort of time and money taken in resolving the leprosy problem. As A M Cooke (1972, p 828) observed in his classic history of the College in the Victorian period, ‘except for obviously absurd remedies, committees were formed, and careful inquiries made’ into almost every other leprosy cure or treatment recommended to the committee. Daji’s photographic evidence was, then, convincing by the College’s own standards and at least equally compelling to Beauperthuy’s claims, yet it was still overlooked. Treated as a mere ‘curio’ from India, they were eventually categorised in the College’s ‘art’ collection, rather than alongside the scientific ‘evidence’ which composes the leprosy survey archive. Although the RCP’s archival collections are replete with examples of patient photography, Daji’s images are the only photographs of patients found in the ‘art’ collection. While it is almost impossible to determine when or why this categorisation occurred, the fact that the Daji collection remains ‘art’ reinforces a colonial hierarchy of knowledge which saw these Indian images as interesting only for their aesthetic qualities, rather than representing the ‘facts’ of leprosy.
Conclusion: photographic uncertainties
https://dx.doi.org/10.15180/211501/005Transported from Bhau Daji’s private practice in Bombay to the hallowed halls of the Royal College of Physicians in London, the photographic images and watercolours of Daji’s leprosy patients sit in a dense web of colonial concerns. Edwards (2014) argues that it is necessary to critically ‘read’ colonial images and ask ourselves what purposes the photograph would have served at the time. The uncertain nature of photographs means it is necessary we have an attunement to who procured them, why and in what socio-cultural context they would have been received. What do we see when we look at the Daji pictures? Is it what Daji wanted us to see: incontrovertible proof of his cure for leprosy? Or is it what the Victorian Royal College of Physicians saw – a curiosity, probably unfounded, like so many other dubious cures for the disease. The images are ambiguous; they conform to the typical posts and representations of ‘other’ bodies in colonial medical photography of the period, and at the same time challenge the often-dehumanising way that indigenous bodies were shown in clinical images. Daji represents an intermediary figure – a learned scholar of ancient Indian traditions and part of a new emerging class of western-trained medical practitioners. Despite his best efforts to conform to the standards of knowledge set by Milroy and the RCP, his hard-earned photographic evidence of his cure was not taken seriously in his lifetime. While there has not been time to discuss it here, interesting comparisons might be drawn to the obfuscation of Indian inventors and intermediaries in the development of other forms of visual technology in the British Raj, for example in the history of fingerprinting (Anderson, 2004, p 167).
The Daji collection of photographs and watercolours at the RCP Museum is a testament to the expertise and medical innovations of Bhau Daji in the treatment of leprosy. The images’ inversion of the traditional hierarchies of seeing typically associated with medical photography in colonial settings make them an important case study in a growing critical literature on the complex role of photography in imperial history. Additionally, they reflect an important period in medical history; one in which considerable confusion around leprosy’s aetiology existed and overlooked individuals sought to fill that gap. Crucially, they attend to the ways that metropolitan ‘centres of calculation’ like the RCP sought to know peoples and diseases across the empire and the way this information was filtered. Photographs may have been a convincing form of evidence, yet what mattered was not necessarily the information they conveyed, but how trustworthy the respondent was considered in metropolitan hierarchies of knowledge. A discovery by a French physician was addressed with considerable interest and expense; that of Daji, despite his association with an elite European medical school, was treated only as a curiosity. Even the supposedly ‘objective’ scientific photograph was only treated so when accompanied by a slew of other materials, data and ‘reputable’ actors.
We hope that re-enlivening the photographs and their place in the history of leprosy and the history of the College itself might serve as a call for the institution to reflect on its colonial history as it again begins to broaden its global reach (Royal College of Physicians, ‘Charitable Aims’). Furthermore, this collection history can serve as a reminder that small specialist museums, in particular medical museums, should not see themselves as removed from discussions on ‘decolonising’ collections. We use this phrase here in quotes since, as commentators have observed, what exactly the term means with reference to curatorial and historical practice remains ‘varied and nebulous’ (Behm et al, 2020, p 169). In line with Amy Lonetree (2012), Annie Coombes and Ruth Phillips (2020) and others, we have chosen to interpret ‘decolonising’ in this context to mean critically considering the colonial contexts of the photograph’s creation, reception and retention through research practice. This, we believe, serves as a way of revealing the embedded power structures of empire and promoting greater understanding of the contributions of colonial people to knowledge, especially in the face of the historical erasure facilitated by European archives and museums. As Coombes and Phillips astutely observe, ‘The move to transform museums is one that aims to establish new sites for mutual recognition, healing, and knowing that acknowledge and respect difference and share authority’ (Coombes and Phillips, 2020, p xlix).
By considering the Daji photographs as they exist within the RCP’s collections, we hope to move towards what Amanda Behm calls ‘the important work to…reframe metropolitan, “Western”, elite, ruling sources’ (Behm et al, 2020, p 171). Little, if any, of the heritage displays at the RCP’s Regent’s Park headquarters are indicative of its colonial past – perhaps because of its physical location in London and association with the regulation medical practice in Britain. Yet no matter the subject of specialist interest, and especially in the case of medicine, colonial ways of knowing are intrinsically embedded in our collections due to the very nature of archival collection and preservation. As Sumaya Kassim (2017) has argued, ‘decolonising is deeper than just being represented’ – it is a set of complex ideas and processes that requires structural change. We acknowledge that we have not acted to redress the inherent racial bias of the museum displays at the RCP, the co-option of indigenous knowledge and expertise by western physicians that the Daji collection represents or the broader racism of the museum sector itself (Wajid and Minott, 2019; Coombes and Phillips, 2020). However, the work of exposing the ways in which historical collections are rooted in colonialism, and that this past influences our present, remains work that museum curators, collections managers and record keepers can and must actively take part in.
Tags
Footnotes
References
Authors


Media in article