Curating Medicine: The Wellcome Galleries
Article DOI: https://dx.doi.org/10.15180/201407
Abstract
The curators of Medicine: The Wellcome Galleries reflect on their experiences of creating these significant new displays at the Science Museum in London. After summarising the historical medical displays at this museum, they outline the curatorial concepts behind their respective new galleries to explore the display strategies and processes behind the development of the new exhibits and highlight the significance of some of the objects that visitors can encounter today.
Keywords
curation, History of Medicine, medical humanities, museum practice, participation, patients, permanent galleries, practitioners, users, visitor experience
Introduction
https://dx.doi.org/10.15180/Medicine: The Wellcome Galleries are unquestionably ambitious in scale and scope. Described by the Londonist as being ‘so vast and its treasures so numerous that a decade of perusals might not be enough’, they cover an area equivalent to 1,500 hospital beds.[1] But the sheer size of these displays should not take away from the subtlety and complexity of human experience explored within them. The Medicine galleries do not recount a chronological tale of the progress of science, although human achievements and discoveries are celebrated. Rather, the personal element is emphasised, with the role of the patient placed on equal footing to that of the medical practitioner. This paper reflects on the curatorial choices and guiding principles that informed the creation of these five interconnected galleries.
‘The art and science of healing throughout the ages’: displaying medicine at the Science Museum
https://dx.doi.org/10.15180/201407/002The Science Museum’s medicine collection is one of the most significant of its kind in the world. It was established in the 1970s as part of an agreement to acquire, on permanent loan, the collection of Edwardian pharmaceutical magnate Sir Henry Wellcome. When the transfer was completed in 1976, it effectively doubled the size of the Museum’s collections overnight.
Wellcome’s extraordinarily prolific and sweeping collecting was informed by the ideals of late nineteenth-century evolutionary anthropology. Advocates of the so-called comparative method, epitomised by Victorian ethnologist General Augustus Pitt Rivers, amassed huge numbers of near-identical items in an effort to establish the origins of cultural practices (Skinner, 1986). By the time he died in 1936, Wellcome had accumulated over a million objects – around fifty times as many as Pitt Rivers had bequeathed to Oxford University half a century earlier. Yet his ambition to create an all-encompassing ‘Museum of Man’ to ‘illustrat[e] the development of the art and science of healing throughout the ages’ remained unfulfilled.[2] Many of the items he purchased at auction or had shipped back to London (via a team of agents posted across the globe) were never even unpacked in his lifetime. A fraction made it onto the gallery floor of his appointment-only Historical Medical Museum on Wigmore Street, which opened in 1913. The Museum began its move into the Wellcome Building at 183 Euston Road – now home to Wellcome Collection, the public venue – in the 1930s, before being forced into storage by the Second World War and the subsequent relocation of Wellcome’s pharmaceutical business to that building. The Historical Medical Museum began to be reassembled onsite in 1954 where it remained (in a reduced form) until the late 1970s, when the object collection was transferred to the Science Museum.[3]



Wellcome struggled to define where medicine ended and life began, amassing everything from infant feeding bottles to entire rooms full of weapons. Despite having been extensively rationalised in the years following his death, his museum collection still comprised some 114,000 objects when it entered the Science Museum. There were similarities between the two institutions – the collecting policies of both, for one, owed much to the Darwinian evolutionary model. However, whereas Wellcome had been concerned primarily with origins, the Science Museum ‘use[d] the past to illuminate the present and future’ (Bud, 2010: 250). Anthropology fell outside the latter’s established interests, which had, in the words of the Museum’s former Medicine Curator Robert Bud, embraced ‘a philosophy of celebrating the importance of science through its practical applications [and] laboratory achievements’ (Bud, 2010: 253).
In an effort to bring the collection up to date, our curators undertook a flurry of collecting activity in the late 1970s and early 1980s. Examples of twentieth-century medical technology took precedence, in line with established Science Museum’s collecting strategy. It is fair to say that much of the material collected during this period reflected recent medical history from the perspective of scientists and practitioners rather than patients.
Within a decade of acquiring Sir Henry Wellcome’s Museum Collection, the Science Museum had launched two new galleries to showcase it. For the first time in the collection’s history, a deliberate attempt was made to create displays for the general, as well as the more specialised visitor. Glimpses of Medical History opened in 1980 and was comprised exclusively of dioramas and room sets (many featuring objects from the collection) designed to ‘help the visitor to gain an insight into how it might have felt to be a doctor or patient at other times in history or in other cultures’ (Bracegirdle, 1981: 1).

Glimpses of Medical History
© Science Museum/Science & Society Picture LibraryA year later came The Science and Art of Medicine, which ambitiously attempted to present a chronological history of medicine from antiquity to the modern age. It incorporated some 5,000 objects, in a quarter of the space assigned to the 2019 galleries.

The Science and Art of Medicine
© Science Museum/Science & Society Picture LibraryBefore long, curators began discussing what new medical exhibits could achieve that the early eighties galleries could not. This was partly born out of a desire to display more of the collection – particularly newly acquired material – and give greater prominence to themes that had received only cursory attention in the near-encyclopaedic approach evidenced by Science and Art of Medicine. Curators were also influenced by new scholarship in the history and sociology of medicine which emphasised patients’ experiences (see, for example, Armstrong, 1984; Porter, 1985).
A series of plans for new displays were developed during the late eighties and early nineties, before Health Matters (1994) got the go-ahead. This gallery sought to combine social history and science studies approaches to create a vivid portrait of twentieth-century medicine that made extensive use of archive films and dramatic object juxtapositions to appeal to general museum visitors and to bring patients into the picture (Boon, 1999). These spaces – Glimpses of Medical History, The Science and Art of Medicine, and Health Matters – were the Science Museum’s major statements on medical history when conversations began about the creation of a new generation of displays a decade ago. This time the galleries would be placed at the heart of the Museum’s buildings, rather than being tucked away on the fourth and fifth floors.

Health Matters, ‘The Rise of Medicine’ section
© Science Museum/Science & Society Picture LibraryMedicine: The Wellcome Galleries
https://dx.doi.org/10.15180/201407/003From the outset, the new project team was adamant that these landmark galleries – projected to remain in situ for around 25 years – would be collections-focused, with digital media and interactive displays playing a supporting rather than a leading role. When it came to establishing a content framework, the team opted for a thematic over a chronological arrangement for several reasons. The latter approach adds pressure to be encyclopaedic – which, despite its uniquely generous scope and global reach, the collection is not, and therefore posed the risk of, being read as an uncritical narrative of linear progress. There was also no expectation that visitors would see the entire suite of galleries in a single visit. With this in mind, individual galleries, sections and showcases were designed to have standalone clarity. Indeed, the interpretation strategy hinges on prominently displayed focus (or gateway)[4] objects, whose labels introduce surrounding content while echoing the key messages for that section.
One organisational concept explored in the project’s initial stages was a ‘cradle to grave’ format, with content organised around the human life cycle rather than a sequential history of the discipline. Although front end audience research suggested this approach would help visitors relate to the collection, it proved a difficult fit for some of its richest subject areas – diagnostics, therapeutics, mental health and disability to name but a few – that affect people of all ages. Nevertheless, the ambition to reframe the collection from a personal, patient-centred perspective remained and was instead transferred to the chosen framework of three ‘narrative’ galleries (Medicine and Bodies, Medicine and Treatments and Medicine and Communities) and two ‘spotlight’ galleries (Exploring Medicine and Faith, Hope and Fear).
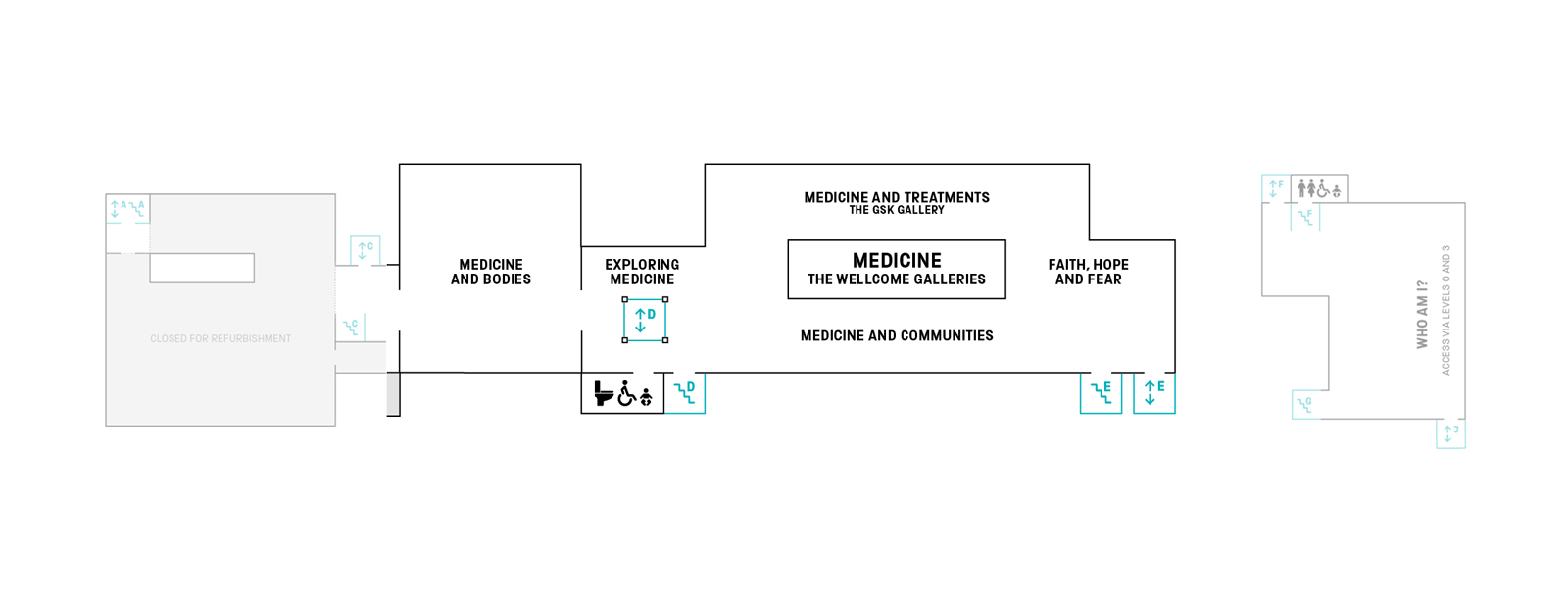
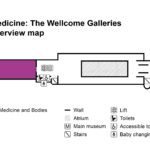
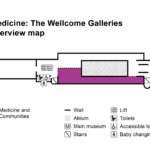
Map of the first floor of the Science Museum (2020), showing Medicine: The Wellcome Galleries
© Science Museum/Science & Society Picture LibraryThe narrative galleries each explore a specific aspect of biomedicine, focusing on the key people, technologies, moments and ideas that have shaped the history of western medicine from 1500 onwards (the areas in which the collection is strongest), while foregrounding perspectives given less prominence in the past. The selected themes were informed by extensive artefact, literature and audience research, with the structure taking its lead from the objects and stories we wished to include rather than the other way around.[5] Occupying the east end of the suite, Medicine and Bodies considers how the search to understand more about the human body has transformed medicine over the last five hundred years, from early anatomical explorations to studying the body under the microscope. Branching to the south of the first-floor mezzanine, Medicine and Treatments concentrates on individuals’ experiences of surgery, therapies and drugs from the perspectives of the people who develop, deliver and experience them, while the neighbouring Medicine and Communities steps back to reveal the health challenges faced by groups, societies and whole populations, from epidemics to the provision of health services and infrastructures.
Visually and conceptually distinct from the other galleries, Exploring Medicine and Faith, Hope and Fear disrupt the narrative format with striking mass displays and a far lighter approach to interpretation. Located at the suite’s intersections, they act as a kind of introduction and coda, showcasing the diversity and sheer scale of the collection. Between them, these two galleries encompass over 1,500 objects from every continent, tracing the many different ways that people have made sense of and managed their health over time and across cultures.
One common thread that runs throughout the exhibition is an emphasis on human experience alongside the technology and practice of medicine. The presence of people, be they patients or practitioners, scientists or service users, is a key characteristic of the 2019 galleries. The team worked with a large number of individuals – all of whose lives had been impacted by medicine in diverse ways – to tell real stories and give a range of perspectives on medicine’s challenges as well as its benefits.
Participation
https://dx.doi.org/10.15180/201407/004Personal stories were unlocked through four participation projects located throughout the suite of galleries. The Science Museum has an established history of using participative practice in both temporary and permanent displays (Boon et al, 2014). Indeed, since the early 2000s, audience researchers have sought to define what participation means for the Science Museum Group.

(top) ‘What is your gender?’, produced in collaboration with Gendered Intelligence and displayed in the Who Am I? gallery in 2014
(bottom) 'Oramics to Electronica'
© Science Museum/Science & Society Picture LibraryInfluenced by Nina Simon’s publication, The Participatory Museum (2010), four broad categories underpin the Museum’s participatory framework: ‘consultation’, ‘contribution’, ‘collaboration’ and ‘co-creation’ (Bunning et al, 2015). Each comprises different levels of involvement and knowledge-sharing between the Museum and its audiences and communities of interest.[6] While all four approaches were used extensively in developing stories for Medicine: The Wellcome Galleries, the participation projects specifically referred to in this article (see especially the ‘Roads to Recovery’ project within Medicine and Treatments) straddle collaboration and co-creation. Each received an allocated budget to finance the delivery of sessions, travel and materials, and was led by a freelance participation coordinator with the support of curators and audience researchers.
Medicine and Bodies
https://dx.doi.org/10.15180/201407/005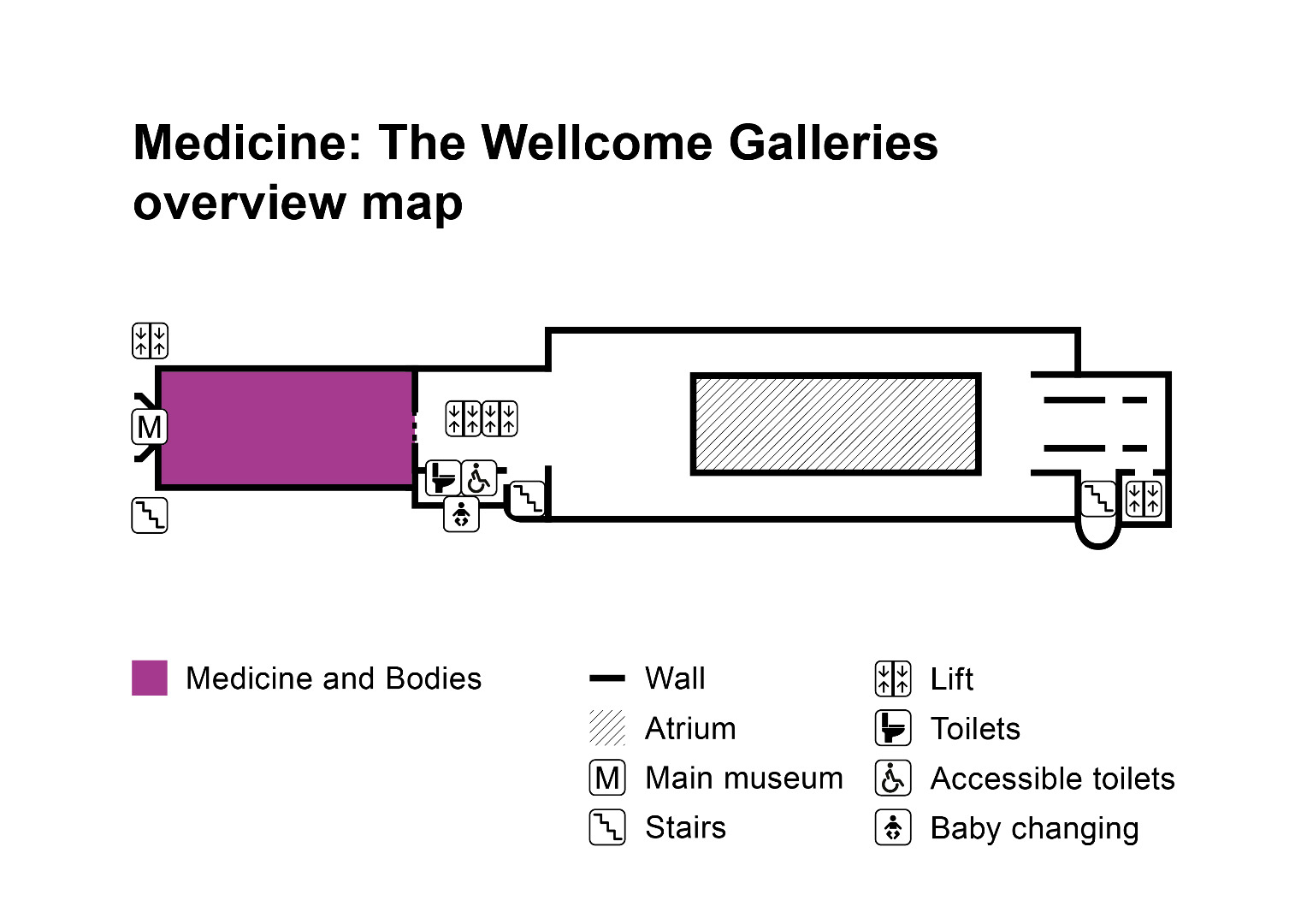
Map of the first floor of the Science Museum (2020), showing the location of Medicine and Bodies, part of Medicine: The Wellcome Galleries
© Science Museum/Science & Society Picture LibraryMedicine and Bodies explores the ongoing endeavour to better understand the human body and how this knowledge has transformed medicine and wider medical culture. The objects and stories displayed within this gallery consider how ways of seeing, understanding and diagnosing bodies over the last five hundred years have come to shape not only medical expertise but also knowledge and expectations about health and illness in wider society.
The gallery explores key developments in medical knowledge across four sections: ‘Studying the Dead’; ‘Imaging the Body’; ‘Measuring the Body’; and ‘Revealing Our Building Blocks’.
Some of the treasures of the medical collection are displayed in ‘Studying the Dead’, including the visceral anatomical models of the Italian sculptor Clemente Susini – wax modeller at the Museum of Physics and Natural History in Florence, known today as La Specola – and French anatomist Louis Auzoux (Ebenstein, 2016).

Wax figures made by Clemente Susini being installed in Medicine and Bodies
© Science Museum/Science & Society Picture Library‘Imaging the Body’ considers how technologies including medical scoping devices, X-rays and scanning techniques have provided the means to see inside living bodies without having to surgically open them. A prominent example on display is one of the very first Magnetic Resonance Imaging (MRI) body scanners, made by Sir Peter Mansfield and his team of physicists in 1978.
All familiar and widespread technologies were once new. One of the narrative threads within this gallery reveals the invention, perseverance and risks undertaken by scientists developing unproven technologies (see Blume, 1992). Often lead scientists volunteer to trial their own inventions at some risk to themselves. When Mansfield offered to be the first person to be scanned using the machine he had built, he had no way of guaranteeing how his body would respond to its strong magnetic fields (though in fact the risk was small). Today, MRI is recognised as one of the safest forms of medical imaging technology and the scans it produces are widely used.

Section view of ‘Measuring the Body’
© Science Museum/Science & Society Picture LibraryThe third section, ‘Measuring the Body’, encompasses some of the technologies and practices that produce quantifiable data about bodies. Familiar everyday diagnostic devices (such as thermometers) sit alongside more opaque, ‘black box’ laboratory machines like the Autoanalyzer, which indicates signs of disease through the analysis of body chemistry, but is normally only encountered by the expert diagnostician. When developing this section, it felt important to challenge visitors’ perceptions of what can be regarded as ‘technology’, which does not always take the expected form of human-engineered pieces of kit. For instance, one exhibit is a Xenopus frog that was widely used to diagnose pregnancy in the mid-twentieth century before monoclonal antibody tests displaced this practice.[7] ‘Measuring the Body’ also addresses research revealing information about the mind, human senses and brain function, examining the patient experience alongside the medical diagnostic equipment. One example is an electroencephalograph (EEG) used by William Grey Walter to reveal patterns of electrical brain activity in patients with neurological conditions. The machine is presented alongside an EEG printout of the first person it was used on at the Burden Neurological Institute in Bristol in 1958. Known only as ‘RC’, the patient was diagnosed with severe epilepsy. Their left temporal lobe was subsequently removed on the basis of abnormal activity recorded on the EEG – a reminder of how profoundly life-changing medical interventions can be.

Gallery view of Medicine and Bodies, ‘Forest of Rods’ model rear, right-hand side
© Science Museum/Science & Society Picture LibraryThe fourth section of Medicine and Bodies, ‘Revealing Our Building Blocks’, examines understandings of medicine at the microscopic and molecular scale. It shows some of the ways that technology has extended the capacity of human observation to reveal the function of cells and the role of micro-organisms and genetics in health and sickness. With intentional contrast to the visceral anatomical models displayed nearby in ‘Studying the Dead’, this section showcases the abstract, architectural models of proteins and other molecules that structural biologists such as John Kendrew, Max Perutz and Dorothy Hodgkin were mapping during the 1950s and 1960s. For these scientists working before the arrival of computer modelling, physical models were critical research tools. They were essential for translating two-dimensional X-ray crystallography images into three-dimensional maps of structures to reveal how a molecule’s form dictated its function in the body. Ironically, this focus on the human body’s smallest units gave rise to some of the largest and most dramatic objects in the gallery, such as John Kendrew’s 1960 ‘Forest of Rods’ model of the protein myoglobin and the replica model of Watson and Crick’s iconic DNA helix.
In addition to objects from the collection, the gallery features a number of interactive digital displays. These were intended to give visitors a sense of what it is like to practice medicine, by offering the chance to listen to lung sounds, explore microscopic images showing the variety of cells within our bodies, and navigate the oesophagus via a gastroscope simulator.
Here and across the suite, it felt important to emphasise how new ways of understanding and interrogating the body using technology did not remain the sole preserve of medicine, but permeated through art, culture and society. The reciprocal relationship between anatomists and artists in capturing and communicating accurate anatomical knowledge is one such area of intersection. For example, visitors can see the gory flayed-skin wax sculptures of the artist Anna Manzolini (1714–1774) who was appointed as lecturer in anatomy at the University of Bologna, an extraordinary achievement for a woman at that time. Elsewhere, the vibrant, avant-garde designs of the 1951 Festival Pattern Group are on show – the product of a partnership between designers and molecular ‘anatomists’ such as Dorothy Hodgkin and John Kendrew, who shared the atomic structures of molecules in the human body that their X-ray crystallography techniques revealed (Forgan, 1998; Jackson, 2008). Rather more prosaic is the pedoscope (a shoe-fitting fluoroscope), which shows how X-rays could be applied to something as mundane as selling shoes on the high street.

Pedoscope X-ray apparatus, by the Pedoscope Co. Ltd., English, 1930–1955 (1988-1332)
© Science Museum/Science & Society Picture LibraryNewly commissioned artworks feature prominently in Medicine and Bodies[8] and are discussed in detail by art curator Katy Barrett in this issue (Barrett, 2020). Indeed, the biggest body on show is the monumental sculpture ‘Self-Conscious Gene’ by the artist Marc Quinn, which greets visitors at the gallery’s entrance. The 3.5-metre statue portrays the model and actor Rick Genest, known as ‘Zombie Boy’, who started tattooing anatomical images onto his skin following his experience of developing a brain tumour aged 15. Through its externalised representations of interior visions of the body, Quinn’s work creates a remarkable encounter at the threshold to the Medicine galleries, evoking a fascination with the body, but also encouraging reflection on the impact that interruptions to health can have on identity.

Gallery view of Medicine and Bodies
© Science Museum/Science & Society Picture LibraryNew art commissions were also developed for Medicine and Bodies through a participation project entitled ‘When Medicine Defines Normality’. Twenty personal testimonies were collected, along with photographic portraits created by the British photographer Siân Davey, to represent the diverse perspectives of individuals who consider themselves – or feel that society considers their bodies – to fall outside medical and social norms (see Sandell et al, 2010). Directed by a core group of participants with personal experiences of sensory and physical impairments and mental health issues, these large-scale photographic and audio exhibits, situated throughout the space, provide a glimpse into patients’ real lives, encouraging discussion about the role of medical interventions in defining health and ‘wholeness’. The images are large, spare and striking, inhabiting the entire gallery floor rather than occupying one small corner. Their presence adds a visible human dimension to a gallery that is otherwise dominated by material things.
In creating the new galleries curators bore in mind the project’s drive to include stories from across society. There was an active attempt here to surface experiences of groups whose voices have traditionally been excluded from history.[9] For example, the collection was reviewed to identify objects that could provide greater visibility to stories about women: as scientists, pioneers, practitioners and patients. One case in point was a group of gall and urinary stones collected from around the world by Kathleen Lonsdale, pioneer of X-ray Crystallography at University College London, and her team. Treated imaginatively, these unpromising vestiges of human pain inspired a visually spectacular display revealing the altruistic motivation behind their collection. Lonsdale was well-known for her molecular chemistry work but was not a medical researcher. She travelled extensively to lecture and visit scientific colleagues, however, and witnessed the health challenges faced by developing countries. As a Quaker, her scientific and social concerns overlapped with her religious beliefs. Towards the end of her working life, Lonsdale became moved by the suffering caused by urinary stones in countries such as India, and pursued research to better understand their composition with a view to preventing their formation (Hodgkin, 1975).
Displaying the stones presented one of the gallery’s most complex mounting challenges. After a lengthy period of sifting through her collection to select calculi of varying size, shape and composition to highlight their diversity, our designers and workshop team created an eye-catching display structure. To overcome the challenge of gravity, conservators crafted individual mounts for large numbers of the stones.

Detail from the Urinary Stones display, Medicine and Bodies, each of the circular depressions display stones removed from one individual
© Science Museum/Science & Society Picture LibraryIn seeking out stories of notable female scientists, the curatorial team also uncovered virus models and electron-microscope slides formerly belonging to the Scottish scientist June Almeida, who having grown up in the tenements of Glasgow (leaving school at 16), went on to become a leading electron-microscopist who pioneered the visualisation and study of viruses. This proved a prescient story to tell in the light of the COVID-19 outbreak, as Almeida was the first person to visualise a coronavirus.
Exploring Medicine
https://dx.doi.org/10.15180/201407/006
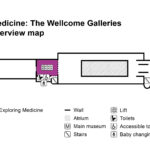
Map of the first floor of the Science Museum (2020), showing the location of Exploring Medicine, part of Medicine: The Wellcome Galleries Exploring Medicine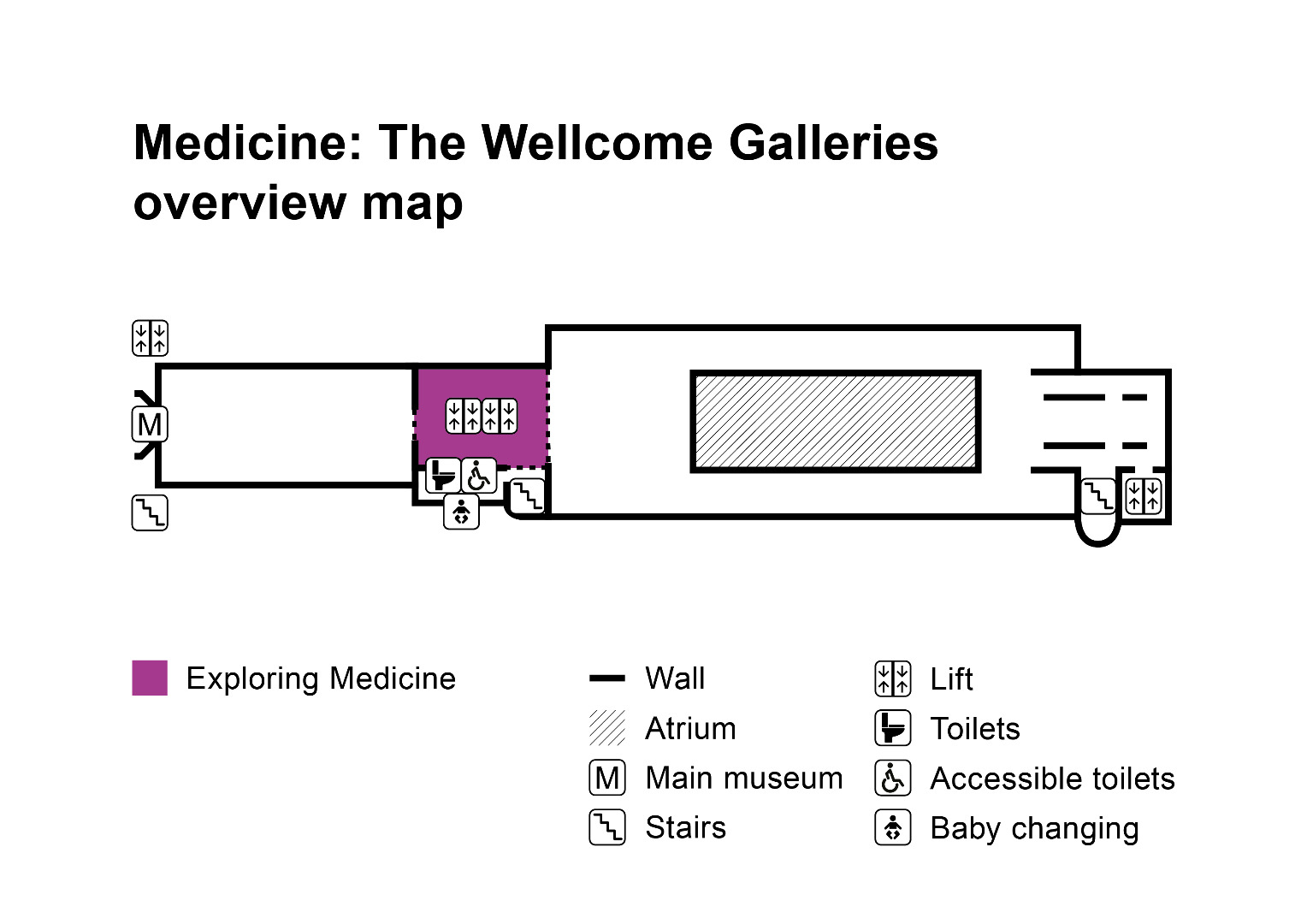

Essentially one enormous display case encircling the Museum’s central lift shaft, Exploring Medicine was intended to transform this space from an empty thoroughfare into a spectacular collection-in-microcosm. Around one thousand objects are arranged in alcoves, either singly or in typological arrays ranging from the highly specific (such as posset pots) to looser categories like masks. When it came to the selection of objects, the curatorial team were seeking to challenge visitors’ preconceptions of what ‘medicine’ looks like, encompassing Wellcome- and Science Museum-acquired material to achieve a balance between the extraordinary and familiar, clinical and domestic, ancient and modern, and objects from a variety of medical traditions, including western medicine.

Gallery view of Exploring Medicine
© Science Museum/Science & Society Picture LibraryWith so many objects on display, it would be easy to overwhelm visitors with information. Instead, only fifteen objects in the display incorporate a label; the vast majority being interpreted via a nearby pick-up gallery guide. This style of presentation has its advocates and detractors; critics fear that displaying large amounts of material with little or no labelling (as was conventional in the nineteenth century) risks alienating audiences, who, lacking the specialist knowledge that would enable them to make sense of what they are looking at, may respond with indifference or frustration (Ames, 1985; Thistle, 1994). Others have made the case for displays that draw visitors’ attention to the objects first, arguing that this encourages active learning and promotes imaginative responses to collections (e.g. Lord, 2005; Dudley, 2010). Here, some artefacts were grouped according to similar themes and practices to provide a non-textual entry point to less familiar material. For the most part, however, the urge to categorise by chronology, geography or theme was rejected in a conscious effort to convey the idea of a collection that can never be fully known or made sense of. The hope was that by separating text and objects, visitors would be emboldened to explore the latter more closely and wonder about the untold stories they hold. This gallery was also intended to act as a springboard for live interpretation in the form of tours and facilitated object handling sessions led by staff, volunteers and invited guests, allowing for more in-depth interrogations into specific topics and histories not represented in the wider galleries.
A summative evaluation of Medicine: The Wellcome Galleries has yet to be carried out owing to the short and interrupted period in which they have been open to the public, but preliminary feedback conducted in February and March 2020 indicates longer than average dwell times in comparison with other permanent galleries. The small number of tours we have been able to offer have proven popular, and observation of visitor behaviour in this gallery – including groups conversing, observing at length and even sketching – are encouraging in relation to the aims and learning outcomes established at the outset.
Medicine and Treatments
https://dx.doi.org/10.15180/201407/007
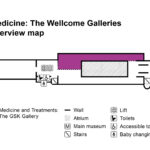
Map of the first floor of the Science Museum (2020), showing the location of Medicine and Treatments, part of Medicine: The Wellcome Galleries
© Science Museum/Science & Society Picture LibraryMedicine and Treatments covers an area of storytelling that is perhaps one of the most familiar to visitors, focusing on individual experiences of medical treatment as well as the people and technologies encountered along the way. Over twenty stories are featured within the gallery’s three sections: ‘Inside Surgery’, ‘Rethinking Treatments’ and ‘Our Journey with Drugs’, reflecting some of medicine’s most enduring therapeutic interventions. When developing this gallery, it was important not to equate treatments with cures and to also consider symptoms, side effects and risks. Stories relating to lifelong and chronic conditions such as cystic fibrosis were included, as was the impact of thalidomide on a generation from the late 1950s and early 1960s.
The content of Medicine and Treatments was shaped by several factors: the Museum’s collection, key moments in the history of medicine and a commitment to tell authentic, personal stories. The project team’s own experiences were also influential, which is perhaps unsurprising when dealing with an emotive topic such as medicine. Yet, there was a desire to look beyond our existing knowledge bases to gain information, expertise and objects from the people who knew these topics best – be they surgeons, historians, manufacturers or members of the public. The decision to use participatory practice to inform and develop gallery content was therefore critical, as was ensuring that featured individuals, with their consent, were visible within the space.
Throughout this gallery people are often represented in their own words, via the use – for example – of large-scale quotations to introduce stories on display and to convey patients’ experiences, such as what it feels like to have a pacemaker implanted for the first time. Quotations also feature on labels, where they are employed to present different perspectives on controversial treatments like electroconvulsive therapy, and reveal lived experiences of practitioners – ranging from neurosurgeons and anaesthetists to technicians working in the instrument sterilisation units buried deep within hospitals.
While individual experience was foregrounded within stories, visual representations of people were notably absent. To counter this, we commissioned a series of six life-size portraits by the photographer Siân Davey; a continuation of the spare style and human scale presentation of her work in Medicine and Bodies. Distributed along the gallery’s spine, they populate the space even when it is empty. Designed as standalone exhibits, each reflects the decisions made by individuals about their health and bodies or the health of others.[10] Each portrait is presented alongside an object relating to the featured person’s story and a quotation about their experience. For Samson Lokele, a surgeon providing sight-saving procedures to nomadic communities in Uganda, it is a question of conducting surgery outside the operating theatre and gaining people’s trust. For Clare Evans, it was the impact of taking multiple medications that sometimes negatively react with each other in order to treat an increasingly complex chronic condition.

Samson Lokele with his on-gallery portrait during the opening events for Wellcome: The Medicine Galleries
© Science Museum/Science & Society Picture LibraryWhile many stories of medical treatments will be familiar to visitors, some of the objects on display in this gallery are more difficult to make sense of. For instance, the Stoke Mandeville ‘bed cycle’ was used by people with partial or lower body paralysis, from the 1950s until the 1990s, when it was donated to the Science Museum. Users’ arms and legs were strapped into the bicycle-like pedals. Via a series of gears, the pedalling motion of the arms was transferred to the leg and foot pedals, providing assistance or passive movement to the lower limbs. Even here, the project team sought to ensure that people and their bodies were visible on gallery so that visitors could engage with how this object worked and how it might feel to use it. To facilitate this, a silhouette of a person (printed on the graphic panel behind the object) appears to ‘lie’ on the bench to provide a visual clue as to how this strange-looking object was used.[11]

The Stoke Mandeville ‘bed cycle’ on display in Medicine and Treatments
© Science Museum/Science & Society Picture LibraryWhere personal stories were lacking in the existing collection, we acquired new objects and accompanying narratives, capturing testimonies first-hand via oral histories and short films where time and budget permitted. One such story reveals the first ever use of 3D printed MRI scans to plan a kidney transplant for two-year-old Lucy Boucher from her father Chris. The printed models were donated to the Science Museum by Pankaj Chandak, the surgeon who developed the concept.[12] The Boucher family, together with Chandak, took part in a three-minute film discussing their experiences, which is displayed alongside the object.
In other areas, participatory work with specific communities was needed. There was a desire to portray a holistic and long-term view of treatment, including the emotional journey of recovery from life-altering conditions such as acquired brain injury. Chronic illness is poorly represented in the collection, and relevant objects often fail to convey the extended and repetitive process of recovery when presented in isolation. Working with people with lived experience was essential to build a fuller picture of what life is like following serious injury. The resulting project, entitled ‘Roads to Recovery’, involved handing over editorial control to a group of six individuals, all based in Yorkshire, who had experienced brain injury.
There were precedents within the Museum for this kind of participatory approach and the team were keen to learn from them.[13] In a previous temporary exhibition, Wounded: Conflict, Casualties and Care (2016–2018), a key exhibit entitled ‘Not All Wounds Are Visible’ was co-created with a group of veterans who had experienced post-traumatic stress disorder following military service in Afghanistan.[14] The group worked with the Museum to produce an object display and film exploring their experiences; this format provided a workable blueprint for ‘Roads to Recovery’.

‘Not All Wounds Are Visible’ display in Wounded: Conflict, Casualties and Care
© Science Museum/Science & Society Picture LibraryOver the course of two years, Participation Co-ordinator Katie Gonzalez-Bell led 22 sessions with the group, adopting similar methods to those used by curators to develop gallery content. Key messages were agreed upon and used to inform object selections, reflecting what participants wanted visitors to take away from the exhibit. They also collectively shaped the narrative arc of a seven-minute self-narrated film sharing their experiences. It begins with their memories of hospital at the start of their road to recovery, before moving on to the challenges they faced and individual goals they have achieved – from putting on their own socks to learning to drive – and concludes with their hopes for the future. Filming included individual studio interviews and on-location shoots with participants’ friends and family. Consent forms were signed at the end rather than the beginning of the process, ensuring that participants were happy with the final edits.
Photograph of the participation group for ‘Roads to Recovery’, at Daniel Yorath House, Garforth The ‘Roads to Recovery’ exhibit in Medicine and Treatments

Creating a sense of place was a technique used throughout the gallery to anchor people’s stories in settings that potently evoke the interaction between patient and practitioner. This approach has a long history within museum display and was a hallmark of one of the Museum’s former medicine galleries, Glimpses of Medical History (Insley, 2013).[15] In Medicine and Treatments, this was achieved in various ways. Images on label strips, environmental graphics and occasionally the objects themselves – such as a LEGO© model of a radiotherapy room – were all used to allude to place.
The gallery is book-ended by two familiar places of medical treatment: the operating theatre and the pharmacy. Both were in fact transferred from Glimpses of Medical History, after audience research carried out in 2014 identified them as two of its most popular exhibits. Richly detailed and populated by mannequins, the sets evoked empathy with people in the past and reminded visitors of their own experiences of surgery or visiting a pharmacy. Visitors were frustrated, however, by the lack of narrative and opportunities to become more involved in the scenes. The pharmacy’s interior was protected by a two-metre glass barrier, which left little room for groups to gather. There was also a reluctance to read labels associated with room sets. The static approach of the 1980s displays contrasted with visitors’ expectations of more dynamic, lively and interactive museum experiences. These insights allowed the project team to tailor how the spaces were re-presented in the new galleries and in 2015, AllofUs, an interaction design and user-experience agency, was commissioned to help explore the digital possibilities for each room set.[16]
An ambitious scheme to show an operation in progress was proposed, delivered via multiple screens in combination with the historical objects featured in the original installation. In the project’s early stages there was a desire for the operating theatre to double up as a flexible event space, building on the occasional use of the 1980s set for live surgical re-enactments.[17] Due to budget and space constraints, however, these plans were stripped back. The end result is a more streamlined, atmospheric display acting as scene setter and visual attractor. Core objects from the 1980s display – lights, operating table and trolley – are accompanied by a 2019 soundtrack recorded at a London hospital. On an opposing plinth sit three hospitals beds originating from different periods, loosely evoking a ward. Brightly lit – in stark visual contrast to the neighbouring Exploring Medicine gallery – and enveloped in a metal curtain recalling clinical settings, the space signals the east entrances to Medicine and Treatments and Medicine and Communities, which branch to the left and right of the first-floor mezzanine.

(top) The 1980s open heart surgery room set in Glimpses of Medical History
(bottom) The stripped back operating theatre in Medicine: The Wellcome Galleries
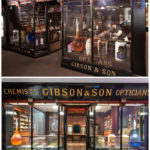
© Science Museum/Science & Society Picture LibraryThe recreated Gibson’s pharmacy is situated at the west end of Medicine and Treatments and looks much like its 1980s incarnation, but has been digitally augmented to create atmosphere and deliver hands-on interaction.

The Gibson pharmacy in Glimpses of Medical History (top) and Medicine and Treatments (bottom)
© Science Museum/Science & Society Picture LibraryServing the town of Hexham, Northumberland from 1834 until its closure in 1978, the pharmacy’s journey to the Science Museum began with a chance encounter by the then Keeper of Medicine, Brian Bracegirdle. He had heard news that Gibson & Son was closing and approached owner John Gibson to see what might be available to the Museum, with a view to recreating a pharmacy for Glimpses of Medical History. Following a period of correspondence, the pharmacy jars, counters, cabinets and shelves were removed, catalogued and carefully packed for their journey south. The Science Museum’s workshop team created a faithful replica of the shopfront was created by the Science Museum’s workshop team, as elements of the original remain protected in situ under the English Heritage Act.

Peopling the pharmacy in Glimpses of Medical History
© Science Museum/Science & Society Picture LibraryMannequins appear infrequently in Medicine: The Wellcome Galleries. While popular with visitors, their use can be problematic for various reasons, not least their tendency to date a gallery very quickly. Different ways of peopling the space were needed. Inside the 2019 pharmacy, visitors can hear a soundtrack (triggered on entry) voiced by actors playing the roles of customers, as well as the pharmacist, Mr Gibson, and his apprentice, Alice. Ambient noises including street sounds, footsteps, a chiming clock and a door bell also serve to create atmosphere.
Touch was an important mode of audience access in the pharmacy given the hands-on nature of making medicines. On a replica counter-top, three items commonly used in turn-of-the-century pharmacies are on open display – a poison bottle, a pill cutter and a pestle and mortar (all purchased or made specifically for the purpose). Using animated projections from above, the countertop becomes a touch screen surface for interactive storytelling, taking visitors through the use of each tool. Two of the objects are accessible to wheelchair users, with an induction loop provided for users of hearing devices and a large print transcript of the audio content available.
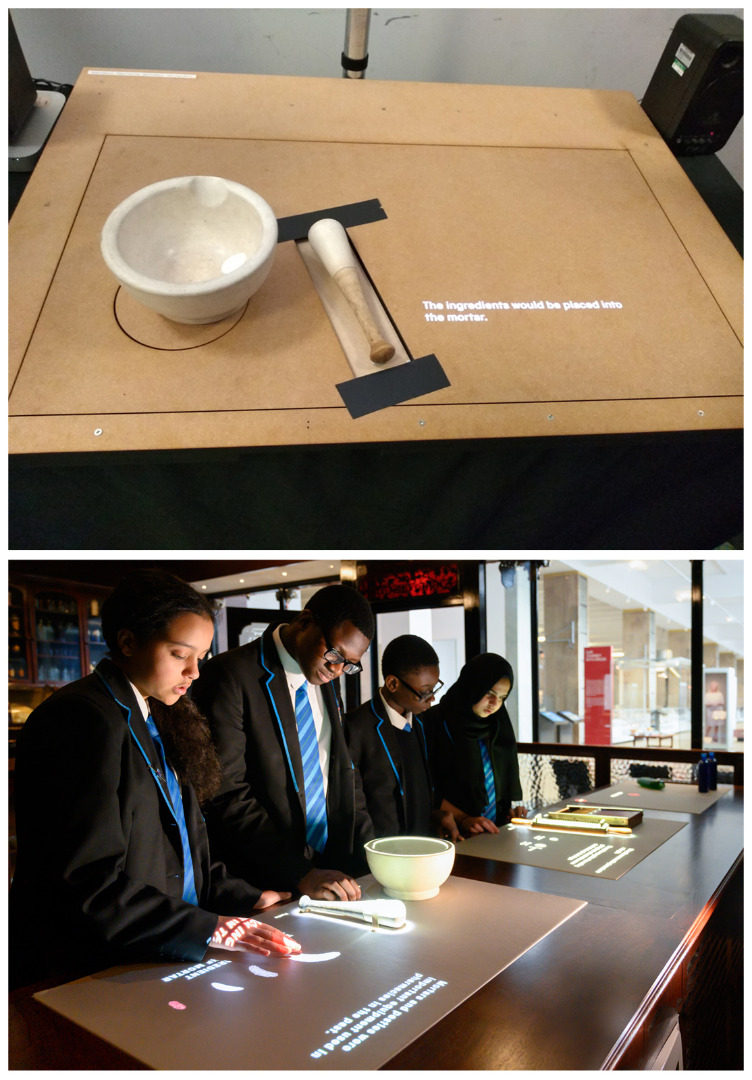
(top) Prototype of the interactive pharmacy counter for audience testing (Credit: Selina Hurley)
(bottom) Students from Petchey Academy exploring the 2019 pharmacy
© Selina Hurley / Trustees of the Science Museum, LondonMedicine and Communities
https://dx.doi.org/10.15180/201407/008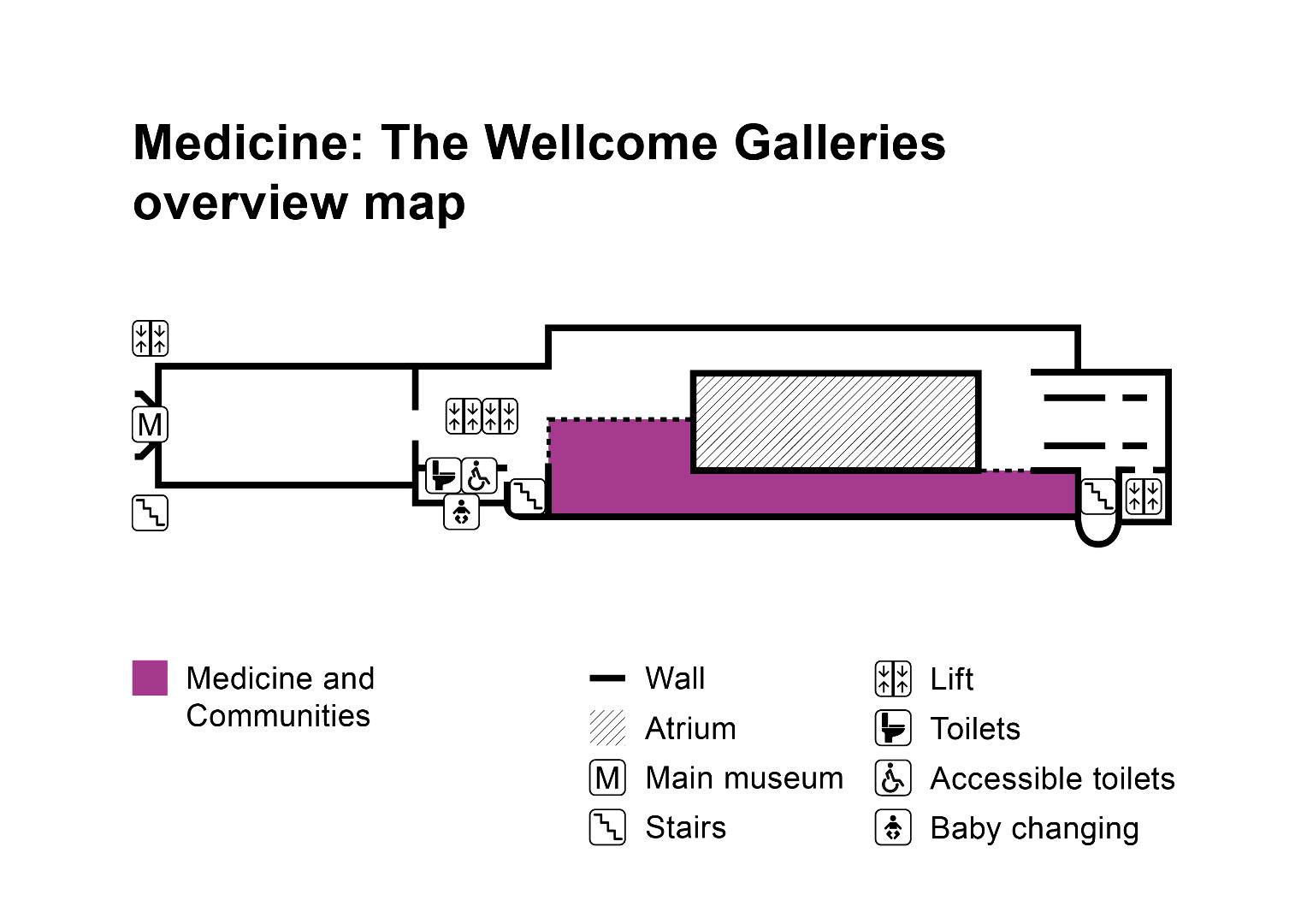
Map of the first floor of the Science Museum (2020), showing the location of Medicine and Communities, part of Medicine: The Wellcome Galleries
© Science Museum/Science & Society Picture LibraryMedicine and Communities zooms out from individual stories of patients, practitioners and scientists to consider how ill health and responses to it have affected groups, communities and populations. The broad focus of this particular gallery is public health, but that does not mean personal health is absent. While ideas around prevention feature strongly, treatments are also present, as indeed they have been throughout the history of public health practice.

Medicine and Communities
© Science Museum/Science & Society Picture LibraryThe gallery is divided into a series of four distinct, yet overlapping, sections: ‘Centres of Care’, ‘Factors for Health’, ‘Fighting Infectious Disease’ and ‘Medical Isolation’, within which the collection is used to illustrate a number of themes. Although this is a gallery about people, on the surface individuals appear to be largely absent. Nevertheless, Medicine and Communities is imbued with a very human character.
Creating displays that primarily deal with the health of populations presented contradictory challenges. Some related to the very different scales associated with population-based medicine. While public health measures can be intimate, such as a (literal) shot in the arm, many are impersonal – like the slogans of campaign posters or public information films that might be seen by millions. Either way, they may often appear to visitors to have little to do with medicine directly, and in terms of their materiality can range from solid permanence to the fleetingly ephemeral. A traditional route to improving community health, for example, is to build a sewer system. Such a task feels more of an engineering rather than a medical feat and hardly suitable for museum display. A very different strategy would be a nationwide letter-drop to inform the public of a specific health threat – as was recently the case with COVID-19. From the start, the curatorial team wanted to ensure that this range and variety of interventions could be properly explored in the gallery. This was achieved through a careful selection of objects – incorporating both the unexpected and the everyday – juxtaposed with still and moving imagery.
There was also the question of how to convey to visitors the size of many public health activities. Early in the gallery project, different forms of interpretation were considered, such as digital graphics, photography and film to suggest the sheer masses of people that can be involved. However, curators were keen that the Museum’s collection would be the emotional focus of the new displays and searched for opportunities where the objects themselves could evoke the humanity needed at the heart of this gallery. The artefacts selected for this purpose were infused with a personal and very human presence but, in keeping with the themes being addressed in this specific gallery, had qualities that spoke of the anonymity of masses of unnamed individuals (Emmens, 2020).
Various examples of this combination of the human and anonymous can be found throughout the gallery. A simple one was employed in a display looking at state-controlled nutrition through rationing. Rather than display a single iconic ration book, as was first proposed, the plinth is covered with them – one from each year of rationing.

Ration books on display in Medicine: The Wellcome Galleries
© Stewart EmmensAll were used by real people and carry their names, but the observer does not need to know anything more about these individuals – even if further information were available. They are instead presented as books that belonged to everyone and anyone.
Wear and tear on objects was also a useful way to evoke personal connections. Physical evidence of use is a familiar characteristic of museum collections and is often considered a problem when choosing material for display. Yet scuffed edges, dents and scratches can provide an affective and tangible connection to the person (or indeed group of people) who once used the object, as well as evoking continuous use over time. Another showcase features scrubbing brushes, a water baler and a drying platform from a public washhouse once situated in the East End of London. These objects appear to have been used almost to breaking point, but their dilapidated condition evokes the many hundreds of unknown people who borrowed them over the years. Of course, they would not have appeared so worn for the entirety of their working lives, but a pristine set would only serve to illustrate function and not have been nearly as effective as conveying the presence of people.

Heavily used bathing implements from an East End washhouse on display in Medicine and Communities
© Stewart EmmensHowever, biographical details and images of named individuals are not entirely absent from this gallery. A number of scientists, public health reformers and health workers are highlighted, but compared to approaches taken elsewhere, these are scarcer. This was deliberate, offering a different approach to the neighbouring Medicine and Treatments gallery where the individual patient voice is central.
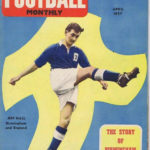
The handful of citizens whose stories are foregrounded from the masses are generally those who have had an impact – often inadvertently – on the health of the wider population. These include Jeff Hall, the young Birmingham City and England footballer whose unexpected death from poliomyelitis in 1959 had a huge influence on the adult take up of the polio vaccine in the UK. Other examples are Joseph Meister, the first recipient of Pasteur’s rabies vaccine, and bacterial ‘super spreader’ Mary Mallon (widely known as ‘Typhoid Mary’) – an asymptomatic carrier identified as the source of numerous fatal outbreaks of typhoid.
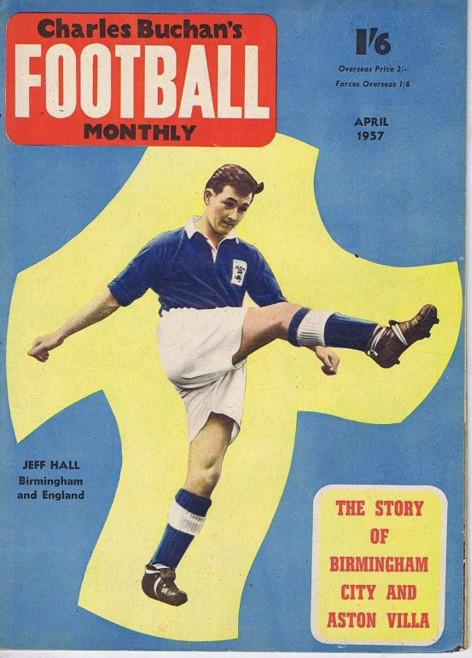
Cover star Jeff Hall two years before his untimely death
© Stewart EmmensThe section most visitors will encounter last is entitled ‘Medical Isolation’. It explores some of the circumstances in which people have been separated from the bulk of the population, often forcibly, on what have been defined as medical grounds. There is particularly compelling content here with which to evoke – even subliminally – individual lives and experiences.
A powerful example of this appears in the displays looking at life in psychiatric hospitals. Here visitors can hear the real but uncredited voices of former patients as they enter a space mimicking the dimensions of the actual padded cell installed alongside it. Then there are the domestic objects from several of the enormous Victorian-built psychiatric institutions which were acquired by the Science Museum when they began closing in the late 1980s. The rapid decline of this nationwide network of institutions prompted curators to collect in this field before historic material was lost.

Life in a psychiatric hospital as displayed in Medicine and Communities
© Stewart EmmensSome of these objects illustrate the work performed by residents in such hospitals. For example, the well-worn spade, shepherd’s crook and straw sun hat used at the in-house farm of what was once the Suffolk District Asylum, and the iron and linen basket from its laundries. But there are also objects that reflect personal hobbies and crafts. There is no record of which resident made the cigarette case shaped like a piano, or who painted the picture of the Suffolk asylum and its grounds, but in this context it does not matter.

A cigarette case (left) and framed painting (right), created by residents of psychiatric hospitals
© Science Museum/Science & Society Picture LibraryAlongside these more everyday items are a number of cast iron grave markers. These had been removed from the graveyard of a former psychiatric hospital that was being converted into luxury flats with a golf course on its grounds. The Museum acquired a handful from the large number stacked up and awaiting collection by a scrap metal dealer. Grave markers exist to identify who is buried beneath, even if the name is eventually forgotten like those on the ration books. But these markers do not carry names, only a number, testifying to the most invisible of lives. They are poignant reminders of how the lives of real people, their identities long lost, can be touched, directed or entirely controlled by public health strategies.

Numbered grave markers on display in Medicine and Communities
© Stewart EmmensFaith, Hope and Fear
https://dx.doi.org/10.15180/201407/009
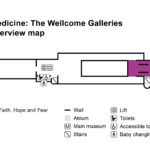
Map of the first floor of the Science Museum (2020), showing the location of Faith, Hope and Fear, part of Medicine: The Wellcome Galleries Faith, Hope and Fear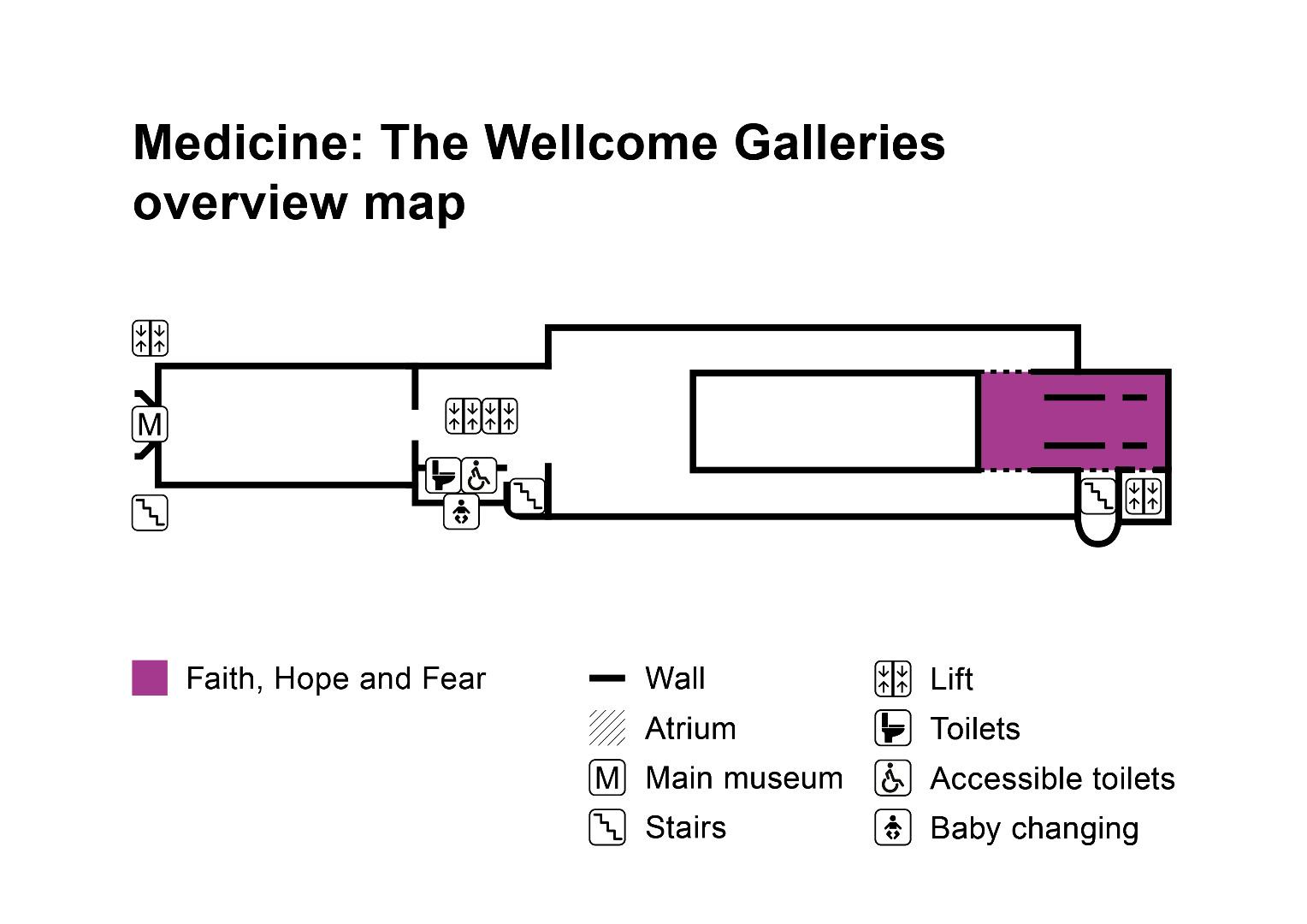

Located at the far end of the gallery suite, Faith, Hope and Fear considers the emotional impact of illness and recovery and shows some of the sources individuals turn to for help when their bodies fail them. The decision to create a gallery about faith in the Science Museum (or the ‘F’ word, as it became known) was certainly bold – not least given the criticism the organisation has attracted in the past for its presentation of indigenous medical traditions and systems from the perspective of contemporary users and practitioners.[18] As the surgeon and public health researcher Atul Gawande astutely observed (2002), however, medicine ‘is an imperfect science, an enterprise of constantly changing knowledge, uncertain information, fallible individuals, and at the same time lives on the line’. As the pandemic has unfolded in recent months, his words have been brought into sharp relief, highlighting the enduring role of faith (or lack of it) – in scientists, the healthcare system, one’s god(s), one’s government – when confronted by a mysterious and frightening new virus that is only beginning to be understood.
For millennia, people have sought moral and spiritual explanations for illness, particularly when it occurs for no apparent reason. The Wellcome Collection reflects this innately human phenomenon, chronicling diverse global healing practices ranging from masquerade and divination to prayer and pilgrimage. Faith, Hope and Fear was an opportunity to display some of these remarkable objects, including votive offerings in the shape of body parts, vessels of ‘healing’ water, statues of saints and deities, and over a hundred amulets. Objects from a range of cultures and time periods are grouped according to type, with the emphasis being on what they have in common rather than what sets them apart.

Anatomical votive offerings and receptacles for ‘healing’ waters on display
© Science Museum/Science & Society Picture LibraryMany relate to life stages associated with heightened emotions and bodily changes such as puberty, pregnancy and death, as well as illness and accident. Instead of debating efficacy, the project team took the decision to emphasise the universal concerns that inspired their creation and use: the desire to identify the causes of symptoms and to do something to alleviate them (even when there is very little one can actually do). The hope at the planning stage was that, instead of asking themselves whether or not a particular approach ‘works’, visitors would empathise with others’ motives and reflect on their own relationships with medicine.

Some of the thousands of amulets amassed by Sir Henry Wellcome
© Science Museum/Science & Society Picture LibraryHowever, the team were conscious that while visually powerful, the Wellcome-acquired objects are partial in the sense that they have long since been separated from their original contexts, owners and stories, as well as dating from periods in history when medicine could achieve far less. Not all visitors will be familiar with the practices they represent, and there was a risk that they would be seen as belonging to medicine’s past. It was therefore vital to include contemporary voices, paired with objects or artworks donated by people who had invested their trust in biomedical and/or traditional practitioners and treatments as well as in spiritual and religious forces. Each of the six stories that appear on gallery represents a highly emotive and ethically complex topic, including IVF, pilgrimage and complementary medicine, as well as areas of biomedicine – such as neonatology and oncology – in which decision making around benefit verses risk is far from black and white. There was not space to examine every angle of these subjects, nor did it feel right to do so using the ‘museum voice’. Instead, visitors are presented with a single poignant object, displayed in a full-height showcase set into an alcove. As they step over the threshold, a voice recording of the donor introduces their own story. The aim was for this to feel like an intimate, privileged experience, hence the recesses that create an air of privacy, while on a practical level also housing the speakers and providing some protection against sound bleed.

Investment: Tabitha’s Gown by Tabitha Moses, one of six contemporary stories featured in Faith, Hope and Fear
© Science Museum/Science & Society Picture LibraryOne topic it felt vital to address in a series of galleries dedicated to medicine was death and dying, but this proved difficult to do using objects. Palliative care, in particular, was something we wished to highlight, being one of the youngest western medical specialisms, and one of the few that explicitly combines clinical care with social, psychological and spiritual support. After consulting with experts in the field, it became apparent that death, while universal, is hugely personal and the team did not feel comfortable presenting a single perspective. Instead, a range of speakers were interviewed including clinical and non-clinical caregivers and community representatives, as well as a person facing the end of his own life.[19] The audio recordings unpick the question of what makes a ‘good death’, asking what support can, or should, be given to people who are dying, how much control it is possible to have over end-of-life experiences and what it is like to live with a terminal diagnosis, along with the impact that modern medicine has on the way people die. The recorded interviews were inset in benches next to a newly commissioned sculpture, ‘Santa Medicina’, by Eleanor Crook. Crook’s fictional surgeon-saint symbolises the hope humanity instils in medicine, and the fear we experience despite our trust in those treating us.[21]

‘Santa Medicina’ by Eleanor Crook
© Science Museum/Science & Society Picture LibraryWhile science may have transformed expectations of medicine, faith continues to play a fundamental role, not least because of the desire individuals have to personalise or take ownership of their experiences. Many people employ a pluralistic approach to manage the unpredictability of treatment, combining mainstream medicine with complementary therapies, elements of formal religion and folk beliefs. Faith, Hope and Fear exposes this complexity, providing space for reflection on the limits of medicine as well as its successes. The legacy of COVID-19 will inevitably shape how this, and all of the Medicine galleries are received, having disrupted so many lives. Unrestricted access to friends and family, primary healthcare and communal religious worship – to name but a few – can no longer be taken for granted.
Conclusion
https://dx.doi.org/10.15180/201407/010With the new galleries intended to serve for a generation, what are the medical curators’ priorities for the future of the collection? While the content framework for Medicine: The Wellcome Galleries was heavily informed by the existing collection, the most recent iteration of the SMG Collection Development Policy has in turn been influenced by the approaches outlined here, and the knowledge and partnerships developed over the past eight or so years. Our core mission, to reflect the role of science, technology, engineering, medicine and media in shaping our past and future, remains, but greater emphasis has been afforded to capturing the personal experiences of makers, users and practitioners, particularly those whose voices have been excluded from the Science Museum’s collections and displays in the past. Contemporary and digital collecting have been identified as priority areas, with targeted projects within medicine proposed on global health issues including tuberculosis, HIV/AIDS and inherited blood disorders, health activism (building on the success of a 2019 contemporary collecting project on menstruation),[21] and chronic conditions, including those relating to lifestyle and an ageing population.
Recently the team’s energies have been concentrated on capturing and recording the COVID-19 pandemic, undoubtedly one of the most challenging collecting projects of our careers. Like many cultural institutions, we have struggled to define the parameters of the task, given the pandemic’s impact on almost every aspect of our lives. This significant and unexpected collecting project takes place within a uniquely difficult set of circumstances. With the entire team working from home since the Museum first closed to the public in March 2020 (four months after the new galleries opened), the curators have by necessity drawn on their personal experience, local and private networks, while being acutely aware of the limitations of this approach. As with the issues encountered in developing Medicine and Treatments, we are balancing the need to represent the scale of the outbreak and the public health measures brought in to control it, with capturing the specific effects it has had and continues to have on the lives of individuals from a wide range of backgrounds. The lack of surviving material culture from previous pandemics has taught us not to ignore seemingly mundane and ubiquitous items, such as flyers and shopfront signage. The rapid pace of the unfolding crisis, however, coupled with the sheer number of organisations and sector bodies involved in the response – not to mention the ethical complexities of collecting during a global emergency – have amounted to a project like no other.
Material secured for the collection thus far include items associated with the medical and scientific response, such as test analysers, ventilators and PPE, examples of advice and guidance produced by a wide variety of sources, and art and design produced in reaction to COVID-19. Specific objects range from lectern signs used at the 10 Downing Street press briefings to Christmas cards and ornaments related to the pandemic and even a pair of wooden spoons sent in by a young family, who broke them while enthusiastically banging pots during the weekly Clap for Our Carers. The vial and syringe used to deliver the first dose of the Pfizer/BioNTech vaccine to 91-year-old Margaret Keenan on 8 December 2020 was also acquired and will be displayed in the galleries when they re-open to the public.

The first vial of COVID-19 vaccine used in a mass immunisation programme anywhere in the world
© Science Museum/Science & Society Picture LibraryFor the curators on this project, the convergence of the experience of developing the new gallery, the drive to instigate more representative forms of contemporary collecting, and the impact of the COVID-19 pandemic has represented a huge step forward in how we think about collecting, displaying and communicating medicine in the Science Museum in the future.
Tags
Footnotes
References
Authors



Media in article