Projecting soldiers’ repair: the ‘Great War’ lantern and the Royal Society of Medicine
Article DOI: https://dx.doi.org/10.15180/201307
Abstract
This article addresses how and why the Royal Society of Medicine (RSM), as a hub of research and education and with its multidisciplinary membership, became active in lantern projection, circulation and popularisation as a scientific teaching practice in First World War Britain. From the interactions it fostered during dialogue to its mobilising of surgeons’ visual experiences and related photographic practices in the facial wards, the article considers how and why the projection services that were made available at the RSM between 1914 and 1919 facilitated collaborative and contested debates in immediate exchanges of information and thus early intervention. Despite the lantern and the camera being referred to in conjunction with each other during this historical moment, the role of photography via magic lantern technology has not been the subject of an in-depth study. During the war, the lantern was received as an extension of photography and toward successful simulation of the spatial and temporal contingency of human vision. This article charts aspects of the nature and body-machine characteristics of these technical innovations in a period of change and transition for both surgical practice and visual technologies in medicine. Overall, the article will argue that the RSM was a major institutional catalyst for First World War uses of the lantern in surgery, producing modern medical thinking that wished to use the camera apparatus in new ways.
Keywords
education, facial surgery, First World War, lantern slides, lantern technology, media practices, medical photography, Royal Society of Medicine
Introduction
https://dx.doi.org/10.15180/In 1916, Harry Baldwin, President of the British Dental Association, addressed 300 members and fellows and 35 visitors at the RSM. In explaining how the ‘section of surgery’ could ‘establish a working partnership with the odontological section and contribute to the discussion of facial injuries’ (1916, p 64), Baldwin established a role for photography and the lantern within the ecology of ‘the group’s knowledge of the subject’.[1] He thanked four Parisian doctors for their contribution to an exhibition of material on display at the Royal College of Surgeons Museum which showed facial injuries that had been treated in French military hospitals.[2] One noteworthy claim in Baldwin’s address suggests that he thought that French and American slides were somehow different from those taken by British surgeons. Or, rather, his comment that in his meeting presentation he sought to ‘show lantern slides of a few typical cases that have come under my care’ to convey to his audience his personal views of seeing the patients recover from operations, and ‘being aware that the greatest amount of clinical material available to us was to be seen in France’ points towards the recognition that the experience of photography was somehow transforming how he looked at his patients’ treatment and, consequently, how he wished to represent this experience (Baldwin, 1916a, p 64).
In Britain, Baldwin was not alone in drawing a connection between the surgeons’ new experiences of patients and surgery; many other surgeons were similarly commenting on the influence that photography was having on their visual experiences. Since early 1916 a growing body of British odontologists, the first group who could realistically stabilise the conditions of facial injuries, had enthusiastically embraced the magic lantern as it facilitated collaborative and contested debate in immediate exchanges of information and thus early intervention. In the process, these physical projections shaped surgeons’ visual experiences by enabling a new technology-enhanced relationship with the doctor-patient environment in the facial wards. It made sense, in such a historical moment, to refer to the lantern and the camera in conjunction with each other, as surgeons did, using the projected photographic image as exchangeable, and interchangeable for the patient and for the surgeon’s experience. How does our conception of the history of medical photography change when we erase the boundaries between ‘lantern’ and ‘camera’ as interrelated practices?
In recent years, historians of medical photography have been engaging photographic practices as a vital element of scientific education, which involved the critical dimension of learning to make images in an effort to improve understandings of surgery and the body (Palfreyman and Rabier, 2017, p 290), as well as addressing questions of war disfigurement in relation to politics, government and post-war reintegration (Biernoff, 2017; Pichel, 2017; Bate, 2018). Yet, despite the fact that medical photography has been acknowledged in hierarchies of science-based military-medical care in the historical period and notwithstanding the pre-eminence of surgery in visual experiences of medical effectiveness (Fox and Lawrence, 1988, p 53), photographic and lantern practices have remained a marginalised subject in medico-scientific contexts. Conversely, medical historians have, at least until very recently, underestimated the extent to which photography interacted with lantern projection in medical practice. Only Emily Godbey (2000, pp 31–69) has integrated these media technologies, as a hybrid instrument of entertainment and scientific education whose material nature influenced the way asylum patients were reintroduced to communal social activities. Yet while Godbey posits a fluid interchange of shared practices between new media emerging since the nineteenth century, she does not show how that materiality shaped the movement of information or gained medical attention in psychiatry across the United States during this period.
This article aims to address these gaps by questioning photography’s place in the context of medical education and research into the facial reconstructions through magic lantern technology. In this article I borrow from the work of Nicoletta Leonardi and Simone Natale (2018) who write from a cross-disciplinary perspective and have as their main object of inquiry the relationship between photography and other media practices. Focusing on the context of the projection services that were made available at the RSM between 1914 and 1919, I aim to reveal how the communication technologies of the lantern and the camera – the technical infrastructure of the meetings and facial wards – enabled new types of collaborative behaviour (Bate, 2016, p 91–103). Besides their display in lantern projection, slides were easily reproduced in printed material. The Proceedings of the RSM, its twice-yearly printed publication, likewise enabled knowledge sharing and collaboration among many geographically dispersed practitioners – as a centralising authority to organise and circulate the direction of experimental surgeries and motivated by collective innovation.[3]
When cooperation took place in the RSM, the facial wards, and in the Proceedings, patients’ treatments were efficiently transformed into key stages of expertise, allowing multiple participants vying for space within these departments to contribute at different levels of effort consistent with their rehabilitative motivation. First, I show that following the conscription of men into military service in 1916, the realisation that surgical solutions to facial injuries had to be resolved in order to prepare for the uncertainties that further fighting would bring contributed to the desperate need to understand these medical problems quickly. Second, I argue that surgeons conceived of the lantern and photography as group-based, co-produced technologies. Production was group-based because no one surgeon, photographer or department used exclusive rights to organise effort or capture its value, and cooperation was achieved through social relations and managerial directions. The close working relationship between medical staff in facial hospitals allowed surgeons to develop these possibilities in their reparative work partly because of the small, portable handheld camera that was used. If carried in the wards, rather than a studio space, at the patient’s bedside or in the consulting room, the intrusive and disruptive working methods of using a large format camera and tripod, not to mention its technical difficulties, could be avoided and the pre- and post-operative results could be quickly collated.
Projecting surgery around 1916
https://dx.doi.org/10.15180/201307/002As scholars such as Bernard Lightman (2017) and Sarah Dellmann and Frank Kessler (2020) have shown, lantern projections came to prominence across Britain in the nineteenth century as a scientific teaching instrument and as public entertainment.[4] The magic lantern is a technology with a history stretching from the middle of the seventeenth century to the middle of the twentieth, at which point it was widely replaced in lecture theatres and homes by similar forms of projection media (Kember, 2019, p 1–8). It is therefore not surprising that this optical device was highly adaptable and found a place within diverse institutional and performative practices, as well as other media, and has a pervasive presence across countless cultural locations, from the fairground to the schoolroom or church hall (Vogl-Bienek and Crangle, 2016; Eifler, 2017). An apt example of this dynamic is in the RSM, founded in 1907 as a central hub in London for promoting and diffusing the scientific aspects of medicine.
Upheld by the modernisation of its aims and members, the RSM sought to bring together all branches of medicine and encouraged collaboration across disciplines. Thus, 15 separate medical societies in Britain were amalgamated into one compact and influential body, dissolving and transferring their assets and property, and reconstituted into 13 sections to unite the profession (1910, pp 657–58). To be seen as a place of authority within the medical community, cooperation of sections needed to be debated, which necessarily occurred inside the confines of the society and its publication. This intersection and interaction between disciplines helped to eliminate specialisation and subdivision between the departments of knowledge (1911, p 1485).
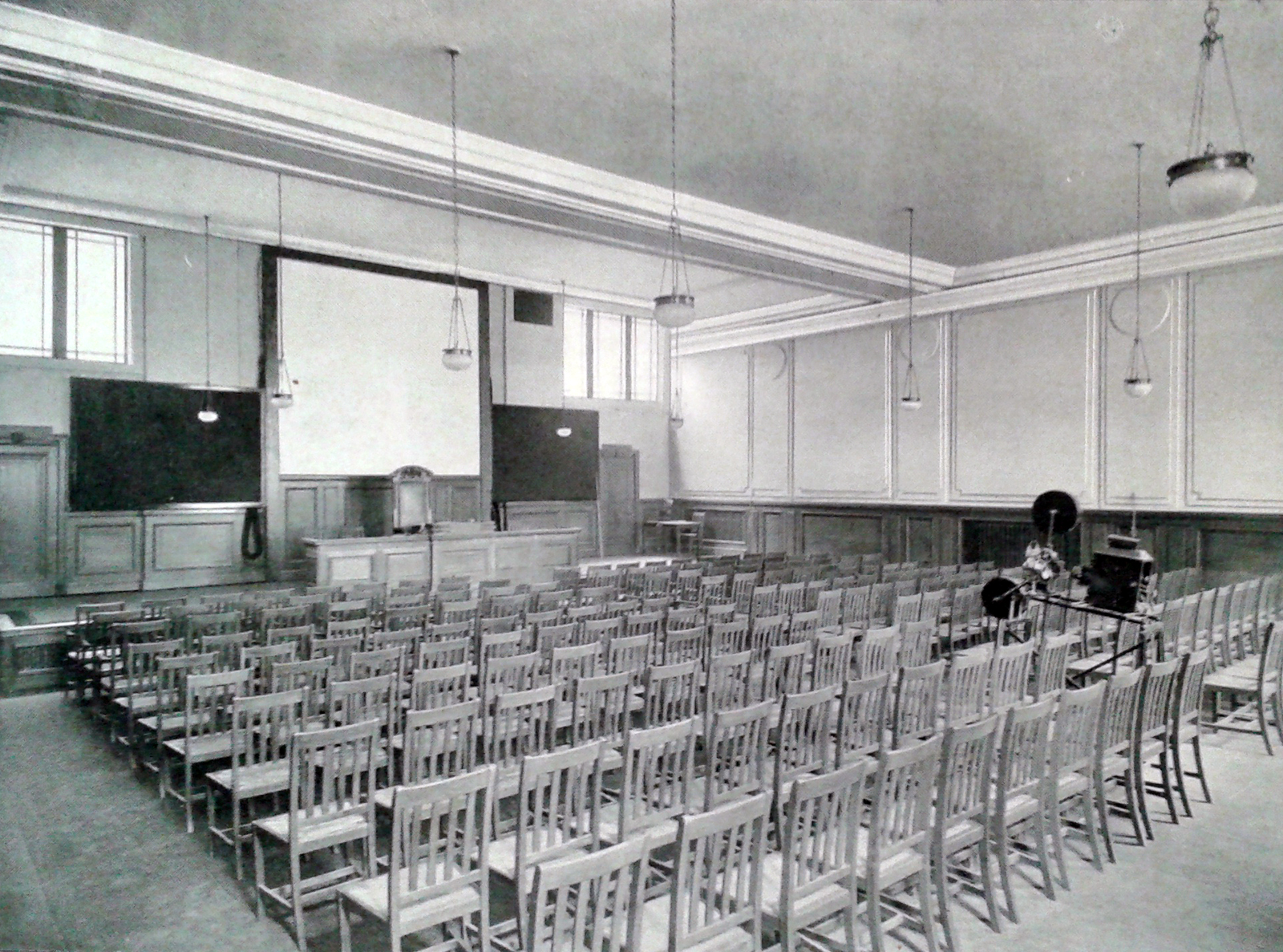
From 1914, the society’s lecture and meeting rooms, at its premises at No. 1 Wimpole Street, were at the disposal of Medical Officers of the Services. Society members found themselves no longer able to avoid ‘the thorny subject of medical politics’ (1918a, p 13). In spite of its hazards and expense, the lantern rapidly gained a footing as part of routine teaching practice within the society.[5] While this fact alone may seem inconsequential, the placement of the lantern at the heart of research debate is not. Weekly evening meetings were crucial so that groups of civilian-surgeons working in face and jaw injury departments for the Army Medical Services could gather at Wimpole Street to perform efficient lantern projections, interact and discuss their experiences, and use sets of slides to present and teach the outcomes of experimental surgeries. Surgeons therefore relied on the importance of physical meetings to explicate new findings of scientific merit and validate their evidence. These weekly dialogues were then extended to the Proceedings by inclusion of speakers’ papers and a selection of the slides.
The images in Figures 2 and 3 show lecture lanterns for both scientific use and amateur home entertainment from the early 1900s, giving a sense of the projectors on the market at the time.
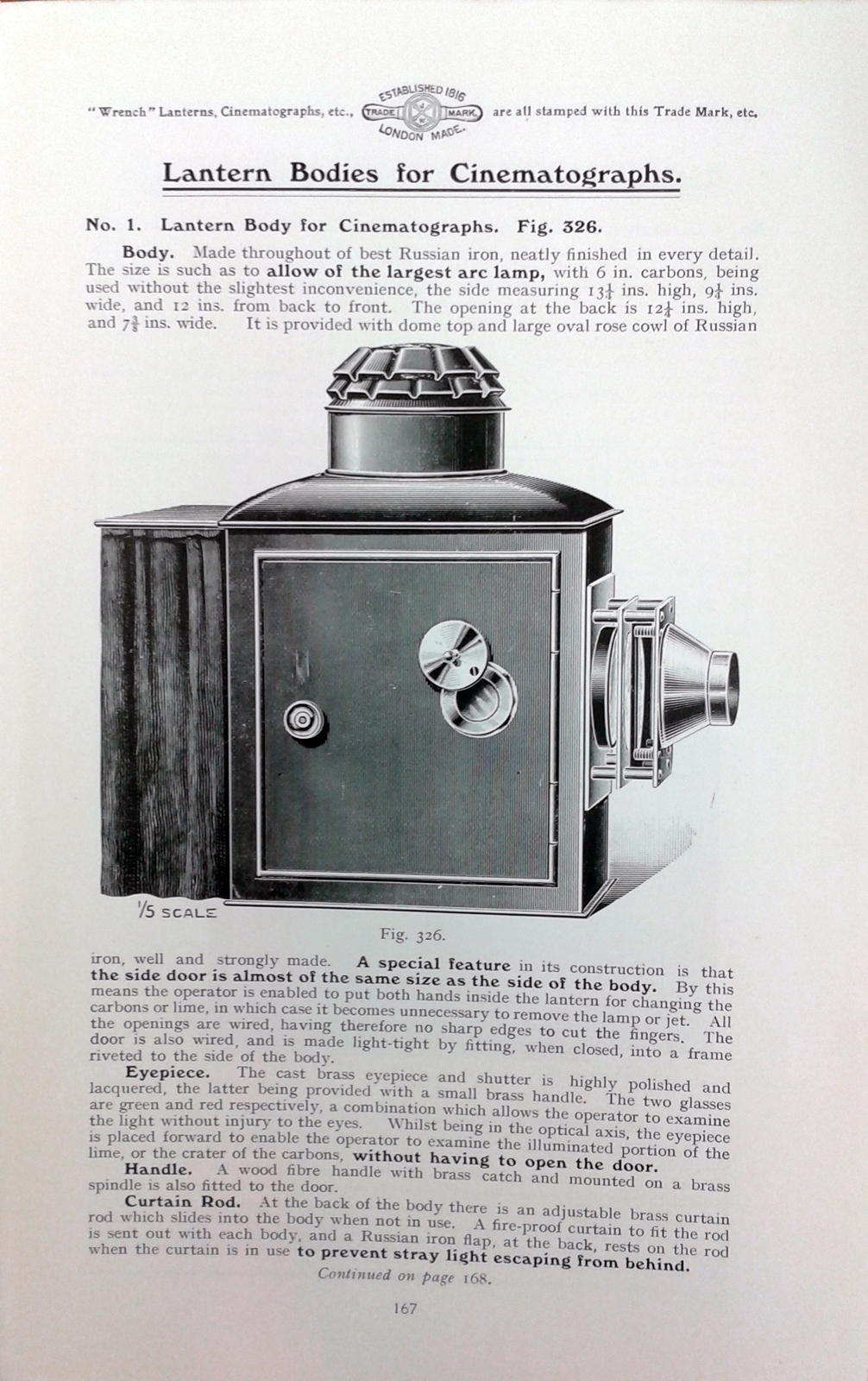
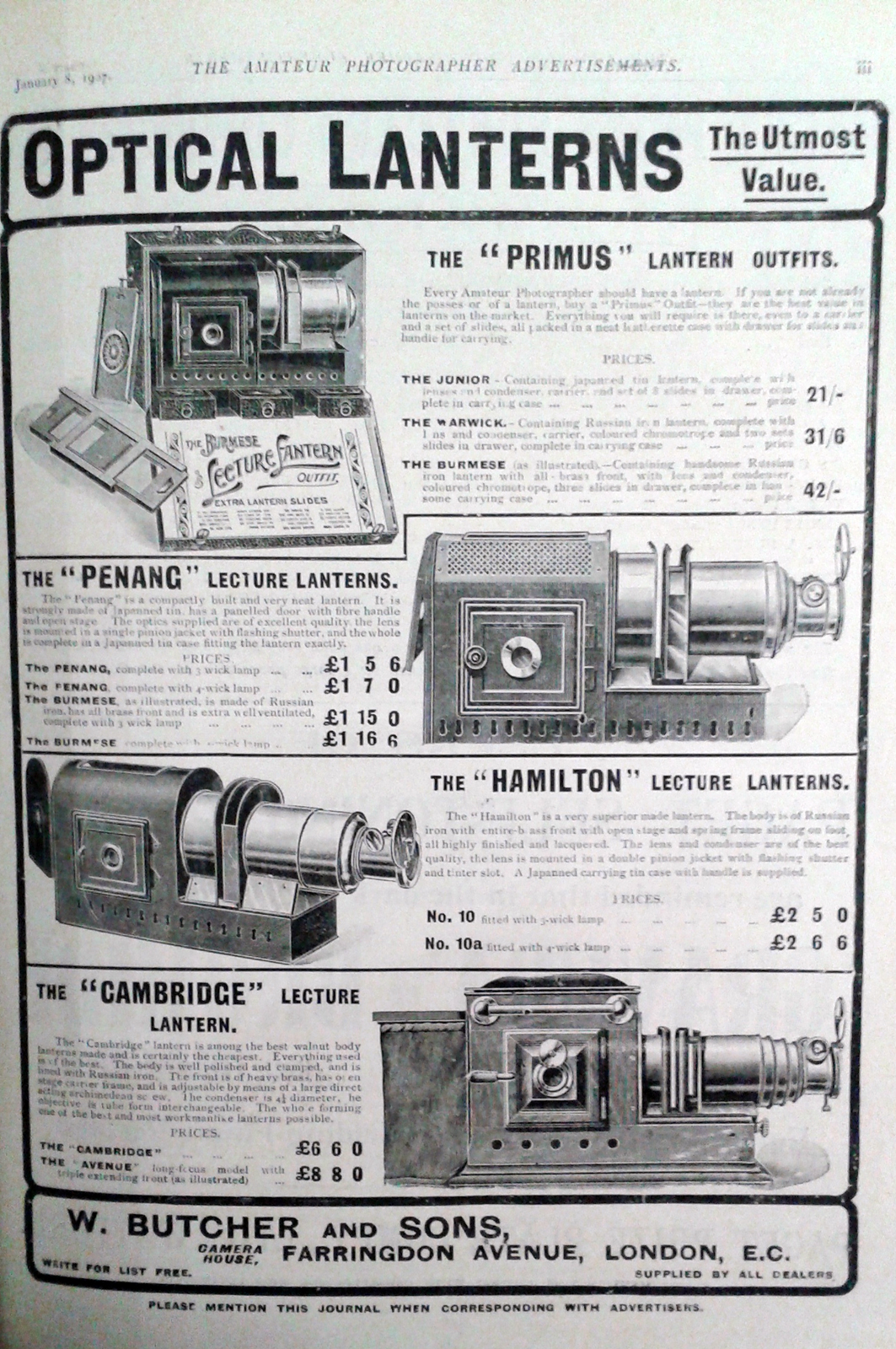
By 1914, electricity was the most commonly used source of power for lantern projections and had replaced older, less reliable and highly flammable means of illumination, such as limelight, oils and compressed gases. In an early history of the electric light for the lantern, published in 1891, Lewis Wright reasoned that electric light bulbs ‘consist[ing] of an incandescent filament of carbon, have lately been applied with some success to the ordinary slide lantern, and where the electric current can be laid on, is a very convenient and handy radiant’ (p 42). In 1878, the American inventor and businessman Thomas Edison was granted a patent for an electric lamp, and in 1883 he joined forces with the Englishman Joseph Swan and formed the Edison and Swan Electric Light Company, and introduced a lamp through which a current being received provided the light source for lantern projection, though it took various forms, such as the new incandescent Ediswan ‘Pointolite’ glow-lamp’ (Wright, 1891, p 39). The innovative nature of the electric light lantern and its safer form of illumination was sometimes underlined by mentioning its relations to the bulky batteries or dynamos, or the availability of supply, and suitable voltage, whether it was continuous, constant or direct. For instance, as Wright explained, ‘the current available from a public supply may be…unlimited so far as our purpose is concerned, and the amount actually used depends only on the total electrical resistance of our circuit’ (Wright, 1891, p 40). In an age when electricity had not yet taken the place of house gas, and a current was still not always available in as simple a form as gas then was, an arc or incandescent lamp had to be carefully selected to match the available current, or the circuit to suit the particular lamp.
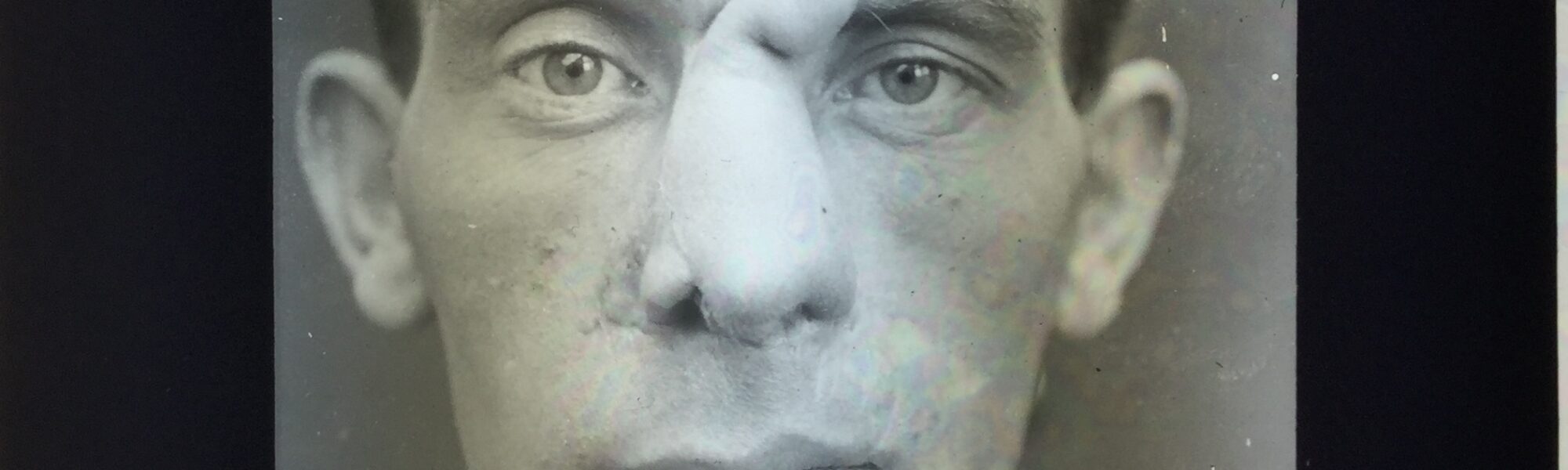
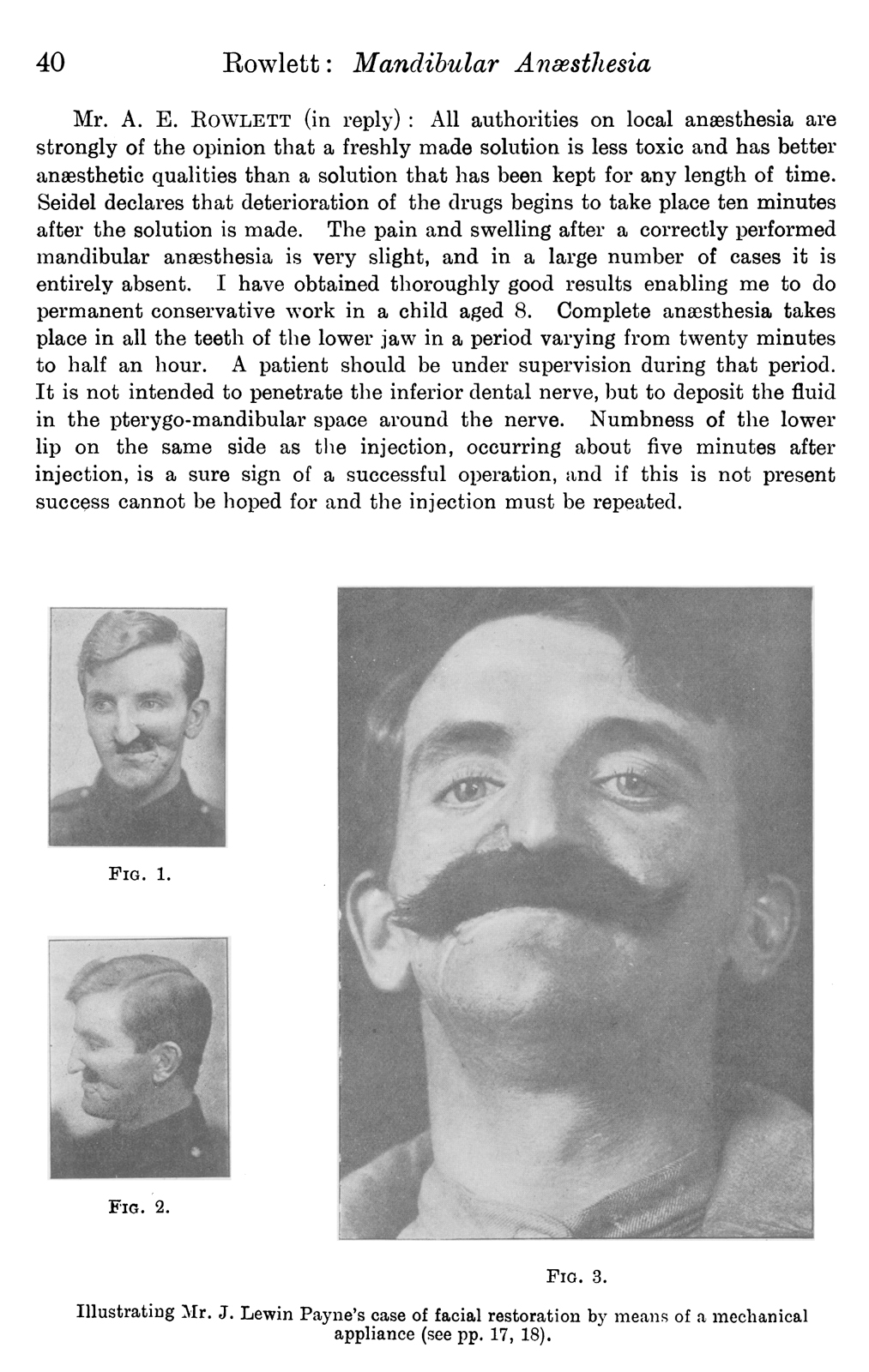
For J L Payne, the innovative nature of the electric light lantern and its safer form of illuminating his slides not only came in the discovery that he made – the physical nature of fractured mandible patients that had come under his care at the Croydon and Wandsworth military hospitals – but also the scientific validity he attached to the images shown on the screen. The opening paragraphs in his article demonstrate the authority of these slides: ‘I propose…to deal briefly with the types of cases met with, the nature of the displacements, the general lines of treatment’ (Payne, 1916b, p 68). This sentence indicates that the images mattered because their production could be traced to his individual experiences of the patients he had seen. This page of photographs shows the side and front face view of a patient who had lost all the anterior portion of his maxilla from the second molar on the left side to the second premolar on the right, with loss of substance to his upper lip and lower portion of the mandible on the left side (Figure 4). After projecting his slides for society members to see, Payne then described what they were seeing: ‘In so many patients there was serious loss of substance, bony union could not reasonably be hoped for; only in the slighter cases was the error in occlusion not likely to be serious’ (Payne, 1916b, p 74). This is an example of how surgeons presented epistemic value through the images to visualise observations of multiple patients and communicate scientific evidence.[6]
Speakers used slides to highlight and explain specific characteristics in types of injury or to contrast the differences in a range of patients, so that others in the room could recognise their nature and comprehend recovery times. Projecting the slide on to the screen allowed for illuminating and enlarging to facial details several feet in diameter. By comparing the photographic results of a range of patients, the surgeon’s performance could point out particular elements of interest on the screen so that others could gain an understanding of the possibilities and limitations of treatment.[7] Visual differentiation not only taught other surgeons how to recognise some of the predictable, and therefore avoidable, problems and complexities in treating these particular injuries in advance, but stimulating such a dialogue also provided access to first-hand experience of these patients to those who had not yet had direct contact or enough experience of their own. Through an analysis of what Erin O’Connor describes as a ‘collapse of the individual…into the identity of disease’ or injury, medical photography renders the person incidental to the portrait and stands in for direct observation itself (1999, p 235). This interchangeable relationship meant that practitioners were taught to read living processes into these surgeries and were given new and immediate proof of the efficiency of these experimentations. The projected images carried enough information for surgeons to assess treatment or to plan-out their own sessions. Photography came to define surgical activity, showing how much skin, muscle or bone surgeons needed to remove or attach in theatre.
There was much professional knowledge to be attained by these projections; words alone never inform the surgeon or trainee of the things most necessary to a safe operation. Learning to read slides in the meeting room involved the full understanding of the procedural stages of an operation. Through the lantern, surgeons harnessed their slides to develop sophisticated visual strategies to portray operative movements and sequencing. As Palfreyman and Rabier have noted, photography and image-making challenged surgeons to rethink their approaches to surgery and body vision, to both master new technologies and instrumentation and to relearn their fundamental skills of hand-eye coordination (2017, p 294). Good teaching comprised the picturing of space and time as well as accessing clinical evidence of the surgical outcomes, so as to piece together the material and the immaterial actions to perceive the invisible techniques, steps and procedures. These dynamic processes of interaction and exchange between visible and invisible matter taught groups of surgeons to venture beyond the boundary of textual communication, into an imaginative and sensory space where mental projection, like the lantern, exposed the steps and timings they wished to recreate to join-up the sequenced ‘moments of observation’ thrown on to the screen.
From cameras to lanterns
https://dx.doi.org/10.15180/201307/003Although taking photographs in the facial wards and presenting a patient’s prolonged course of treatment via lantern technology were clearly considerably demanding activities, the Proceedings encourage us to look at these media in concert with each other, rather than in isolation (Natale, 2018, p 36). In this section I follow this encouragement by pointing to relations between photography and the lantern that legitimised scientific communications during wartime Britain: offering groups of surgeons and departments first-hand accounts of treating facial injuries, reinforcing these accounts by leading the audience through the assessments arrived at, and establishing claims to diagnosis and a justification for treatment. For instance, the shared technologies of photography and the lantern became not only a mediation of the scientific experience, but an extension of the research activity in the specialist centres, as an embodiment which was at once an instrument, an analytical category and a methodological orientation (Riles, 2006, p 7).
The exchange of slides by Payne in 1916, discussed in the previous section, also supports this interpretation of photographic and lantern technologies as an extension of the surgeon’s body as these were not only meant to illustrate or prove the point he was making but also to pose the research question of how to effectively treat the patient. With sets of slides, groups of practitioners could compare their own experiences of patients, the correlating of which helping to elucidate many of the difficult surgical and mechanical problems that awaited solution. Norman Bennett had received under his care similar patients resembling Payne’s ones, with not much loss of bone. The fractured parts of jaw were allowed to consolidate a little before separating them rather than using fixed caps or splints. The cases were also similar to patients that J G Turner had treated. He chose to immobilise his patients’ jaws, with the possibility of regeneration of new bone.[8]
The handheld camera’s lighter weight meant that a larger number of plates could be carried in the wards, and exposures were short enough to allow surgeons or medical photographers to hold the apparatus against their body, and up closer to the patient, without a tripod, which was a bulky and restrictive component of the equipment. This design element in relation to the body facilitated a new portability and visuality in the wards and influenced what surgeons thought of photography and what they came to expect of it. Indeed, Baldwin’s comment ‘to favour nature’s efforts at repair by every means in our power’ suggests that he did not consider his photographs to be sufficient alone in recreating such an overview, something that, we can assume, he attempted to address with the lantern by sequencing the slides in a particular way and by adding his commentary (1916a, p 64). As was the case with many surgeons, the visual experiences that they talked about when they came into the meeting rooms do not seem to match the photographs they took if viewed individually.
Surgeons’ dialogue revolved primarily around the usefulness of photography in advancing the lantern effect. As J L Aymard, a surgeon at the Cambridge Hospital, Aldershot, explained in his article in The Lancet (1917), the point of interest to all surgeons when assessing the grafting technique employed to rectify any deformity ‘is to discard the first photograph, but to examine carefully the one depicting the result of nature’s efforts prior to operation’ (p 891).[9] His justification for this was that the artificiality of photographic vision rendered single photographs inconclusive because he had personally observed patients on a daily basis. To present a photograph of the original condition of the patient and to miss out the second photograph is, the author continued, ‘from my point of view, more than misleading. To the experienced plastic surgeon some of the largest facial wounds which appear sensational before and behind the camera present few difficulties by the time nature has completed her part’ (Aymard, 1917a, p 891). Aymard’s response to the artificiality of photographic vision as a form of physical measurement of surgical repair and the spatial and temporal contingency of human eyesight was to reaffirm the lantern in the interpretation process. If single images were contested, it was necessary for the surgeon to further photography by exaggerating the temporal and spatial dimensions and effects of reconstruction. For Aymard, the lantern effect retrained or redisciplined surgeons’ perceptual habits of surgery and photography. In this sense, slides presented to the audience and reader needed to control the imagination as much as possible, so that the exaggerated sense of space and time was evident and led back to the camera.
The simplified process offered by the marketing of lightweight and easily transportable handheld cameras freed up photographers and surgeons to engage with their newfound visual, portable and experimental independence because of the sensitivity of commercially available extra-rapid glass plates. These extra-rapid emulsions had only just become fast enough to capture a patient’s healing within hours of surgery.[10] This demand for instantaneous photography was widely shared by surgeons and photographers who worked in the facial centres. In 1917, for example, with a flood of patients being admitted to British jaw hospitals and the rapidly escalating need to train surgeons to be ready for them, surgeons produced an even more rigorous photographic practice, which was sufficiently quick to secure good pictures of performed techniques in theatre – observations that implicitly links surgeons’ experience of time and space of the surgical technique and healing process with their photographic desires. By far the clearest articulation of this changed focus is in a presentation Percival Cole delivered to the section of odontology on 3 December 1917.[11] All of the images in his article reflect how the visual value of photographic technologies moved to the service of the projection lantern.[12] Once the patient’s progress was exposed on to the sensitised plate and reconstruction was sequenced and underwent translation and transmission into the slides, the reproductions constituted a visuality of recovery into key stages of treatment and assessment, and opened up, as Orton puts it, ‘new possibilities for algorithmic image calculation’ (2018, p 6). Judging the success of his methods and evaluating his decisions retrospectively, Cole questioned whether he should have postponed the treatment of his patients or operated sooner. He also considered whether a different method would have worked better in light of the facts secured by the slides. In a context where there was a developed and active knowledge community and constant participation, in Cole’s instructions as an operating theatre experience one could see a newly configured visual practice for dental-surgical culture.
Cole was invited to take part in this discussion, and presented to the group several slides ‘bearing on the treatment of wounds involving the mucous membrane of the mouth and nose’ (1918b, p 11). All of the slides in the presentation are also displayed as photographs in the RAMC albums.[13] Moreover, many photographs that ended up in albums were first produced for projection in meeting rooms and read within the Proceedings. The three photographs of the first patient displayed in Cole’s article are laid out in the same order as in the album, although the photographs in the article have been cropped and enlarged during reproduction to focus the reader’s attention to the scarring on the patient’s cheek. Cole then points out photography’s ability to capture, represent and carry this information, ‘pictorially at any rate, its configuration is a more accurate guide to the surgical measures necessary and the result achieved than is the residual deformity’ (1918b, p 12). Cole’s attempt to represent such ambitious grafting techniques photographically constitutes a significant methodological bridge between 1916 and 1917 and a site of the working out of the shifting episteme. Cole presented slides of his patients’ results soon after operation, sometimes within hours. Considering his experiences in relation to the physical mobility enabled by a handheld camera, which sometimes even captured patients before they were strong enough to leave their beds, Cole could share with colleagues a patient’s response to treatment almost immediately. The exchange of these slides became an essential way in which Cole and his colleagues could economise time and labour. With the shear mass of patients being admitted into facial wards, a photographic slide could mean the difference between success and failure. Surgeons could consult their patients and photograph them very quickly, and adjust working methods accordingly, before the next similar case came along.
This eagerness to engage with ‘recovery’ should be understood not simply as a desire to capture and thus carry information on the surgical technique into the meeting room. More importantly, this was a way to negotiate and then modify the information carried by the individual, still photograph, with the personal and subjective vision of the surgeon. Instantaneous photography in the facial wards, which carried an assumption of directness and spontaneity of observation, met the aims of the surgical agendas because it was seen to enable the immediacy of scientific intervention. For surgeons presenting their slides in meetings, the directness and spontaneity of vision of the instantaneous photograph appealed to this new way of seeing and thinking because of the embodied sense of technology that it provided.
The use of the lantern led to an association of touch and sight and temporal and spatial effects of patients and surgeries that seemed palpable even though they were not. The groups of surgeons in the meetings became components in the visual apparatus. Moreover, surgeons utilised this visual apparatus as a tool to lay down fundamental principles of surgery and to advocate an emergency tool kit method that would effectively translate research work into a specifically photographic methodology. The first stage of treatment was when a surgeon should study, research and plan for the operation. The second period was the operating stage when the surgeon would perform a graft or reconstruction in theatre. Then came the third stage; the surgeon did not do anything here, he waited. More precisely, the surgeon was involved in both pre-operative studying of the photographic image of the patient and a post-operative assessment of him, at which point he would comprise analysis of the operation with the slide to determine the extent of reconstruction. The surgeon was therefore involved in both pre-surgery studying of the slide or photograph and in the post-operative assessment of how much had been achieved. The surgeons were continuously asked to assess the progress of their patients while also training themselves to acknowledge the artificiality of the photographic slide and image and while also keeping their normal vision in check.
The practicality of photographing the patient in this context is fuelled by a desire to see where the surgery is going and how the patient is recovering. While the slides and photographs had many uses for surgeons, they were particularly helpful for planning out operative sessions because the activities were of such duration and complexity, and the surrounding areas of a patient’s face were altered so significantly. This led to the need for more photographs to be taken to quickly map other parts of the face, which, in turn, led to the planning of additional reconstructive operations, and to further alterations and the need for new photographs. In that way, photography was a feedback loop in regard to the uncertainties which groups of surgeons felt. This cycle can be traced through the development of the surgeons’ overview of a patient’s recovery. However, this could also take the form of a more complicated process, from a certain view or sequencing there are limits to the human eye sight, such as an oversimplified account of an injury’s functional capacity as time and space is foreshortened or bled into one another.
In the First World War, the discussions of French, American and British practices coupled with a range of innovative surgical thinking and communications, from photography to the lantern. What was the lantern’s place in circulating the results of facial injuries across broader modern technologies of communication and longer-term educational concerns? In what way, then, was the chemical photographic image transferred from live lantern lecture to an ink photograph in a published paper? As the next section shows, examining the combined meetings of laryngology, rhinology and ophthalmology between 1917 and 1919 may provide us with key insights to answer these questions.
From lantern to published papers
https://dx.doi.org/10.15180/201307/004On 1 November 1918, James Donelan, president of laryngology, praised the developments he had witnessed in this scientific field over the last two years (1918c, pp 1–7). Three months later, at a meeting on 7 February 1919, with Donelan in the chair, 13 members of the section of laryngology were carried on a journey through three years of experience caring for patients with combined wounds of the orbit and sinuses by means of lantern slides (1919a, pp 115–147). G S Hett, a RAMC major working in the Ear, Nose and Throat Department at Sidcup, invested his work with visual authority by presenting an extensive set of slides as points of investigation and to verify the systematisation of ideas he and his colleagues had made.
Hett invited those present in the meeting to assess the surgical outcomes for themselves. The group then interpreted and debated these slides, to open for discussion the possibilities of graft and cartilage supports in the rebuilding of these injuries. This meeting was later published and circulated as 20-page and 12-page articles and fully illustrated with 58 photographs for the wider community that constituted the Proceedings’ readership.
Printed in the Proceedings, the ink photographs took on a new meaning that was a constant reflection of their production and their earlier forms of display as photochemical slides in the meetings, as epistemological objects to be conferred. In this way, readers could articulate the lantern at the heart of research debate by tracing the reproductive images, following the photomechanical translation from the ink photograph on the article page directly back to its related item – a chemical positive on glass, and a projection, and allowing a seamless connection back to the pedagogical narrative aligned with the speaker’s individual knowledge (Wilder, 2017, p 386). The value given to a photographic image was made explicit through its reproduction in print. In other words, a photograph gained meaning through the steps and processes of its translation from a slide in a meeting room onto the printed page and through its textual documentation (Foucault, 1973, p 95; Latour, 1999). Elizabeth Edwards and Sigrid Lien’s notion of copy photographs is essential here to understand how these slides, as intermediary analogue copies, became part of a ‘processually invisible layering’ of bureaucratic activity and knowledge formation (2014, p 3).
On 7 March 1919, Hett shared 28 slides of a further seven patients under his care amongst laryngology colleagues. Adding precision to his February paper, Hett ‘sketch[ed] out further principles which he had not yet touched on’ (1919a, p 136). He sequenced his slides so as to replicate his experience of continuously seeing these patients for two or three months progressively improving, projecting ‘before and after’ images for each, including admission shots, newly formed grafts recorded within hours of insertion, and healing times spanning several months. The slides that Hett had projected on to the screen certainly stimulated debate, and reinforced the lantern as a fundamental technology of visual validation for his methods. The group praised Hett’s care for these patients and for obtaining uniform good results. Somerville Hastings, having also treated many such patients, had found it useful to adopt a method of making up the new nose first with wax, before having it recast in metal by the dental department (1919a, p 133). Herbert Tilley interjected with a further option, to use portions of cartilage removed from one patient on the day before it was implanted in a second patient, as long as the piece was kept in sterile saline solution during the intervening night (1919a, p 133). Here the group was using their own personal observations and experience to corroborate the slides and evidence of Hett. Lawson Whale found Hett’s slides striking, for allowing one ‘to see how the scar tissue softens and the colour and texture of the skin approximates to that of the surrounding skin’, and recounting cases that had not proved so successful, he commended Hett’s work in tissue transfer, stating, ‘I made some noses in France earlier in the war, and those which are not lined do not do so well’ (1919a, p 133). Owing to the costs of reproduction, the printing of so many slides was only made possible by Hett’s collaboration with the editorial team, who had to submit a statement of the costs of reproduction to the council committee before publication could be approved.[14] One week after Hett presented his second paper, the council of laryngology met on 14 March 1919, whereon Donelan announced, ‘Mr Hett was willing to bear the cost of the blocks himself’.[15] For Hett and for the Proceedings, the slides acted as an essential part of transporting his personal experiences to his colleagues.
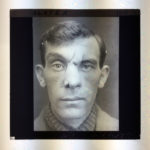
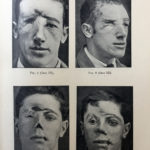
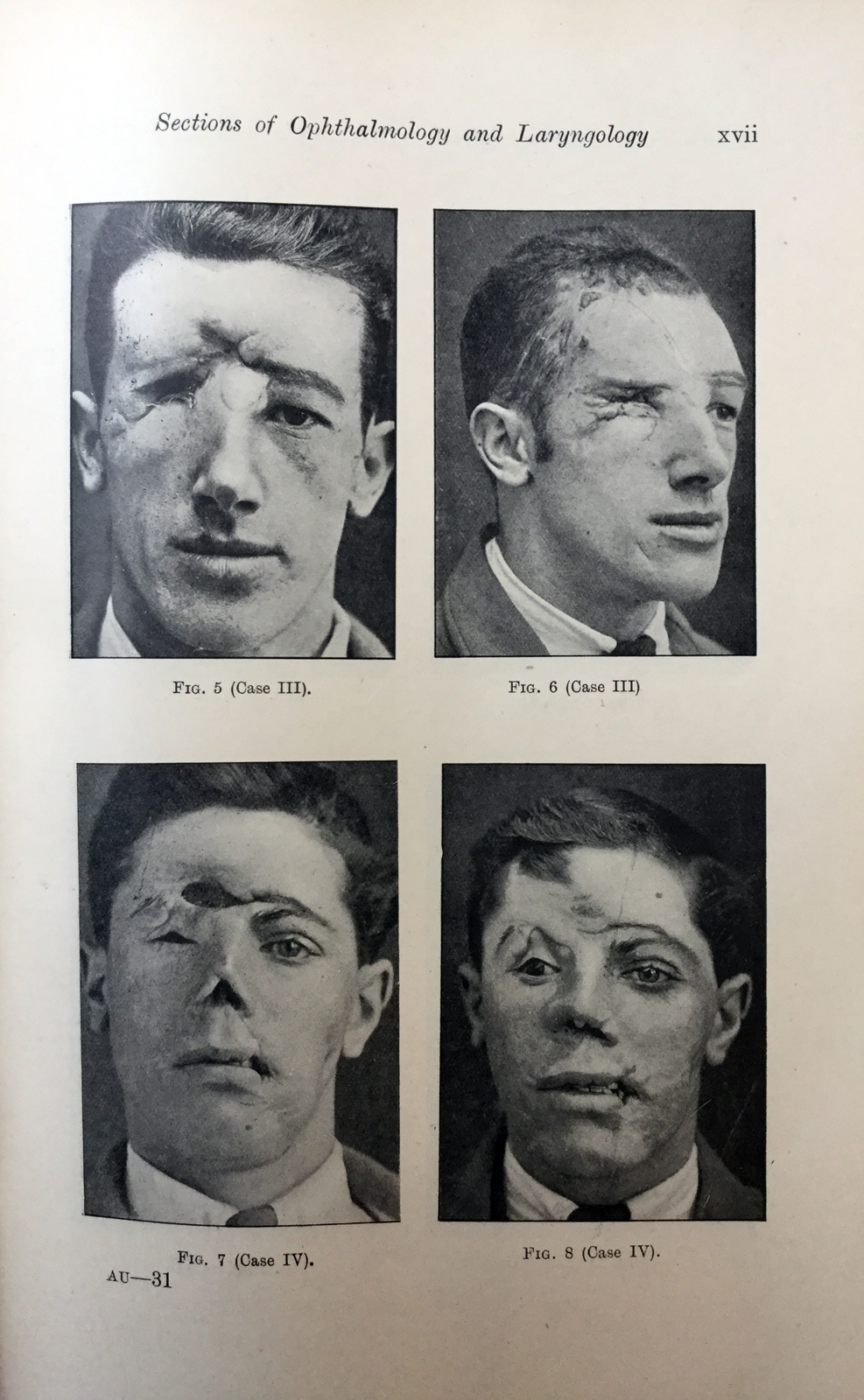
Hett was called back to Wimpole Street to present again on 2 April 1919, this time at a joint meeting of the sections of ophthalmology and laryngology. The ophthalmology section had called this joint meeting out of a desire for new ways to learn about the dangers which beset the optic nerve. The emphasis that Hett placed on the lantern was compounded in this meeting when he projected a total of 40 slides as a topic of debate to bring these practices together. The slide’s value within this meeting lay in the way it posed questions of coordination for ophthalmologists and laryngologists. The first five patients Hett showed had suffered gunshot wounds involving the frontal sinus and orbit (Figure 5):
Case 3 is one in which both frontal sinuses were opened by a wound and the right eye had been enucleated. An obliterative operation has been done on both frontal sinuses and a plastic operation…performed by sliding down a forehead flap to remove the forehead deformity (figs. 5, 6, p. xvii). Case 4 is similar. I have done a plastic operation for the removal of the frontal deformity, and have readjusted the eye-socket so that an artificial eye can be worn. A rhinoplasty was done for the existing destruction of tip and alæ of the nose (figs. 7, 8, p. xvii).
All the speakers at the joint meetings acknowledged Hett’s slides as a shift in the understanding of combined ophthalmic and plastic work. With the experiments carried out at Sidcup, the slides demonstrated to both sections that the treatments should actually be sequenced in a field of action and not performed in isolation. In order for laryngology and ophthalmology cultures to prove to their readership that these images were valid, their argument needed to be one of coordination, and for the articles and images to be read together. This cooperation, a key aspect of their conjoined practices, makes for a distinct reading of the texts. The first two articles from the February and March meetings, which contained in total 18 patients and 58 photographs, provided an in-depth visual analysis, thus targeting a laryngology readership, as well as indicating the purpose of the images to ophthalmologists. This coordination of ophthalmic and plastic arguments was unique at the time, and augments the way they began to interact around all the elements that were connected or mutually implicated in a field of action and being presented to them.
Two additional joint meetings were held in April and the subsequent publications moved further beyond the confines of a single discipline, and the reader had to move across different epistemological boundaries. While these sections of the society were distinct disciplines, in that they were divided into two fields, the discussions in the meetings and articles intertwine. While some of the readers of the Proceedings may have attended the original meetings at the society, others could be equally informed. The slides, allowing the free transit of teaching objects to the journal publications and library open shelves, were entangled in the active training of a much broader audience of society members and fellows through their replication in printed media. The translation of the slide into forms of publication helped to establish their sequencing into courses of treatment and recovery times that could be conceptualised and followed. Thus, reinforcing the scientific authority that was attached to the lantern slides in the original debate, and consolidating their pedagogical significance. As material objects, the Proceedings are able to circulate rules and guidance on facial reconstructive procedures and predicted outcomes. Through a series of slides, publications and albums, it becomes apparent that these facial injury photographs do not just emerge from their negatives and travel on completely disconnected and divergent paths. Wilder is surely correct to underscore the usefulness of thinking about proximity of these objects as they come into contact with one another through catalogues, or on shelves, or in albums or books, as ‘more than a physical attachment, since they influence one another across decades and across collections’ (2017, pp 393–394).
With the absence of slides in most medical collections, due in part to problems with storing large numbers of fragile glass objects compared with the ease of storing and displaying prints in albums or journals on open shelves, the physical absence of these slides is shaped by the practicality of preserving one and not the other – as part of a museum’s ecosystem. The slide’s apparent efficacy in the RSM, its utility within the meeting rooms and how it travelled and was put to work, was valued only as a means of reproduction and not as stable media for storing knowledge indefinitely (Roberts, 2016, pp 319–339). Indeed, as Edwards and Lien argue, the volatility, instability and even disposability of the material forms of photographs, as required by their traditional roles in museums and archives, reinforce this undervalue (2014, p 4). Many institutions such as the Royal Geographical Society and Royal Photographic Society kept their slides and still have vast slide collections, preserved as useful objects for learning and tending to have long lives circulating around classrooms and lecture halls. Yet, the slides from the RSM were transformed by their exit from the meeting room by only being reused in the short term, then later archived and forgotten, reproduced in Proceedings – for ease of collecting, display and access within the library.
Conclusion
https://dx.doi.org/10.15180/201307/005Since the first experimentations with the camera in the facial wards of French military hospitals in 1914 and 1915, the rapidity of patients being admitted into specialist centres produced in surgeons a desire to consult and photograph them very quickly. New findings of reparative work could then be projected and clarified alongside and to fellow members, and also extending out from the meeting rooms in the form of cooperation with the library and the reproduction of slides in the Proceedings. This situated the projector in relation to a visual epistemology and professionalised practice in modern medicine in the early twentieth century. As one article in the Proceedings suggested, such systematised case taking is worth while, and saves its cost over and over again, in that it tends to better results and quicker results, even though an accompanying footnote to this article reads: ‘owing to the costs of production, all illustrations of splints and several photographs shown in the epidiascope have been omitted’ (Northcroft, 1917b, p 8). Among the advantages of knowledge sharing was the creation of common standards of best surgical practice, which would then end up having labour and economic benefits as well as fostering interdisciplinary exchange, just as the Medial Officers recognised.
The practicality of photographic developments like split-second exposure times in the wards emerged at a decisive time for surgeons. The photography this allowed broke with how surgeons saw their work, radically changing ideas about modern maxillofacial surgery. The lantern aimed to further temporal and spatial awareness by broadening the scope of photography: to simulate surgeons’ everyday experiences of seeing the individual changes in a patient’s transformation and to document the healing process. The product of a handheld camera, instantaneous photography seemingly extended the human vision across several months of treatment in the same way in which the lantern was felt to produce the effects of tactile, haptic and even visceral practices that aided a physical and not just a visual-linguistic perception, in order to comprehend the moulding and stitching of flesh, muscle and bone. This allowed surgeons to capture, and thus understand, what the camera could only see as ‘before and after’ exposures, simultaneously inspiring surgeons to think of photography in their departments as sequenced and rapidly changing. The desire to articulate visually this new sense of one’s own presence in the experience of seeing patient recovery influenced the emergence of a modern medical thinking. It sets in play the surgeons’ embodied agenda to give material form to the medical gestures and aftercare performed in the theatres and wards.
Camera and lantern technologies had subjected the surgeons’ senses to a complex kind of training, and this urgent need to comprehend patient recovery times was met by manipulating the spatial and temporal contingency of human vision so that this could be taken in. It becomes clear to see how the conjoined technologies of photography and the lantern during the Great War were part of a larger mediative framework, and one in which medical slides and photographs were not only produced and disseminated but were also part of a surgeon’s process of thinking reparatively, and where surgery was being developed via visual practices, with images and surgeons as an operational aspect of the reconstructive process. Thus, surgeons’ slide-led presentations became a site for communicating feelings of immersion in daily war duties, a form of substitute for personal experience of rehabilitation, giving authenticity to what could have been witnessed. In similar ways to the photographic projections of patients’ regained health, the magic lantern slides reflect the interrelationship between how an image of a patient was exposed with a portable handheld camera and the larger role that it played in communication of new ways of working in the facial wards. In this way, they were visual and epistemological objects moving across time and space and between different media outlets, which took on new meanings of the experiences and temporalities of recovery from the new pace at which this was now taking place.
This endeavour can be understood as satisfying a desire to be able to increase photography’s proximity to everyday visual experience in the facial wards. The precision and unabridged detail of the photograph encouraged surgeons to enrich it with additional elements of visual perception – sequencing. The lantern raised sensitivity to the photography in the wards, unleashing expectations of its practicality and mastery across several months of treatment and intensifying discussion about the spatial and temporal contingency of human vision. In this way, lantern technology encouraged dialogue in the meeting rooms between the two media. The interweaving of changing surgical and photographic practices helps to elucidate how, during the war, the lantern was used to further the process of photography and towards successful simulation of the surgeon’s experiences of vision. In the meeting rooms, groups of surgeons expressed the idea that their medical researches were converging to make possible a complete rendition of their visual experience of the facial centres. Photography and the lantern flourished in this environment because they allowed the creation of sights that would not have existed otherwise.
Acknowledgments
Earlier drafts of part of this article were presented at the workshops A Million Pictures: Magic Lantern Slide Heritage as Artefacts in the Common European History of Learning in Exeter, in 2018, and Photography and Printed Matter at St Andrews University, in 2019. I should like to thank the participants at both workshops for their insightful comments as these helped me to refine the ideas presented. My thanks also to Robert Greenwood, Librarian at the Royal Society of Medicine, London, for his kind assistance in tracing key sources; and to Joe Kember and Phil Wickham for sharing with me their knowledge on the lantern.
Tags
Footnotes
Back to text
References
Media in article