

The valuable role of risky histories: exhibiting disability, race and reproduction in medical museums
Article DOI: https://dx.doi.org/10.15180/201406
Keywords
collections, disability, exhibitions, material culture, Medical museums, mental health, public engagement, race, racial science, sexuality and reproduction
Introduction
Over the last few years medical museums have entered a particularly productive period of renewal and expansion, including renovations of major museums in Austria, Denmark, Norway and the UK, the launch of new institutions in Croatia, Germany and Latvia, and proposals for others under development in Belgium and Spain.[1] In the Netherlands alone (where I am based), the Museum Vrolik reopened in 2012; the Rijksmuseum Boerhaave in Leiden launched a new suite of permanent galleries in December 2017; and the Dolhuys Museum of the Mind in Haarlem is currently completing its second major renovation in six years.
As collections once intended only for medical practitioners or students in training have opened up to a broader public, museum staff continue to debate the risks and rewards of exhibiting medical materials for very different purposes than were originally intended. In this essay, I highlight some of the trends that I consider most important for the future of medical museums and collections, and reflect on some of the challenges they face. I draw generally on my background as a curator of historical exhibitions at the National Library of Medicine in the United States (2002–2012) and my academic career as an historian of medicine, and specifically on a four-year research project I am now concluding on the social relevance of European medical museums.[2] Between 2016 and 2020, I visited 35 museums in 13 countries to interview staff and tour exhibitions, contextualising these examples within the relevant scholarship produced by medical museum curators and academics. I focus here on some illustrative examples from a small selection of medical museums which highlight issues common to many.
The field encompasses a wide variety of institutions with very different profiles, from smaller volunteer-run collections to major publicly funded museums employing a large staff of heritage professionals, some located on medical campuses or former health facilities in remote locations, others within lively cultural areas in the centre of major cities. It would be impossible to draw universal conclusions across such a broad range, and inappropriate to insist that all should take up the approaches I advocate here. Instead, I offer my thoughts on the significance of some of the shifts underway to acknowledge the innovative work already started and to suggest potential avenues for further activity in the future. In particular, I argue that medical museums have an important role articulating and challenging how medicine has defined norms and the ‘abnormal’, in the past and in the present. Cultivating critical reflection on the ways this shapes medical research and healthcare will help to address stigma and discrimination in these realms as well as in wider society.
In contrast to growing calls to remove highly charged objects and topics from display, I propose deeper engagement with these ‘risky’ materials and the histories they represent. In fact, limited engagement with these histories in wider society, and with the on-going inequalities they sustain, has given some materials in medical collections a disproportionate significance. Because the work to address centuries of abuse and discrimination as well as their contemporary manifestations is ongoing and complex, removing objects and issues has become a simple, and in my view insufficient, strategy to circumvent critique. Art has been used very effectively to augment exhibitions, to add the perspective of patients or to reframe the outmoded and controversial ideas and practices some objects represent. Although I appreciate the benefits of this approach, I am also concerned that this trend can eclipse or displace the historical collections, contributing to the diminishing appreciation of their potential for visitor engagement.
The end of ‘cabinets of curiosities’?
https://dx.doi.org/10.15180/201406/001Since the 1980s, the traditional exhibition style of ‘cabinets of curiosities’ has been revived and reinterpreted across numerous museum venues (Lubar, 2018). This trend has continued in many of the renovations of medical museums in the last twenty years.

Re-imagined ‘cabinet of curiosities’ in Wellcome: The Medicine Galleries at the Science Museum, opened in November 2019
© Science Museum/Science & Society Picture LibraryThe approach has provided the opportunity to show a large proportion of a museum’s holdings, and to present artefacts in a similar way to their original, historical organisation and display. Ordered by types of anatomy or bodily systems, or by forms of disease or deformity, the strategy created a spectacular visual impact and incorporated vast amounts of material. Such expansive displays impressively conveyed the major enterprise of collecting, dissecting and modelling that began in the seventeenth century and which has shaped the production of knowledge.
In the aftermath of scandals about the misuse of human remains, and controversies over the Body Worlds exhibitions, medical museums drew on the tradition of cabinets of curiosities to legitimise their presentation of human specimens and anatomical waxes to a broad audience.[3] The wealth of objects on show in crowded cases vividly illustrated the central role of such collections in research and education, but left little room for interpretive text, or for specific attention to each item included. Such displays often implied medicine’s major role in the categorisation of humans as abnormal or ‘monstrous’, in legitimising racial hierarchies through scientific ‘proof’ of white superiority, and in defining women as the weaker sex, although usually without any, or with only very limited, commentary on this history. This also served a very practical problem, given the lack of surviving information about who a specimen came from or how a model was produced.

Cabinets of comparative anatomy including older style in the centre and modern versions either side, installed in the renovated gallery that reopened in 2012 at Museum Vrolik, Amsterdam UMC, The Netherlands
© Paul Bomers, courtesy of Museum VrolikIn the context of a wide range of opinions among museum staff and audiences regarding what should be shown, and to whom, cabinets of curiosities set aside the larger questions of why these objects had been saved, or the purpose of re-exhibiting them today, leaving it to visitors to determine their scientific, artistic, historical or educational value. Such silences have become increasingly untenable. In the first place, attendees have often wanted more information about the things they were looking at, even if the limited information available could only explain what pathology or anatomy the object shows, and why it was scientifically valuable. However, these details reinforce the medical gaze already produced by the mode of display, reducing individual people to representative specimens or cases.
As a consequence of this, as well as the way much of this material was produced and obtained (well before any standard of informed consent was established and often benefitting from a lack of protections for the poor, enslaved, colonised or condemned), today museum staff and visitors view many of these objects as problematic, putting them at risk of removal or deaccession (Richardson, 2001; Sappol, 2004; Claes and Deblon, 2018). This ignores the role exhibition strategies could play in engaging audiences with these artefacts and the histories they represent. Karin Tybjerg, curator at the Medical Museion in Copenhagen has recently argued that ‘the discussion of whether human remains should be exhibited has overshadowed the question of how they should’, and as I suggest here, the problem is expanding to encompass a growing list of non-human material that is also considered too risky, or difficult, to display (Tybjerg, 2019). Yet these objects are valuable precisely because they may generate some of the most intense reactions among audiences.
As I discuss here, focusing on the representation of disability, race and mental health, some medical museums are beginning to reckon with medicine’s role (and medical museums’ role) in defining ‘norms’ and declaring some people, characteristics or behaviours as ‘abnormal’, inferior or deficient. This approach is risky in several senses. By putting scientific authority under critical scrutiny, museums risk antagonising medical organisations and individuals with whom they are affiliated, as well as visitors from the medical profession. By attempting collaboration between different communities of experts who have sometimes been at odds, museums risk clashes between groups and pressure to adopt or suppress conflicting views. Finally, presenting highly contested objects and subjects for public interaction risks alienating audiences and generating controversy and criticism. The third topic I discuss here, reproduction, appears so risky as to be relegated to the sidelines, underscoring the continuing taboos regarding public display and discussion of childbirth, abortion, infertility and miscarriage while simultaneously demonstrating the urgent need to do so. I end by suggesting some strategies that may help to rehabilitate these topics and their material culture in the future medical museum.
Critical histories of medicine
https://dx.doi.org/10.15180/201406/002Museums of the history of psychiatry were the first in the field to re-imagine how their collections could be interpreted to engage broad audiences, including visitors who are highly critical of medicine’s approach to mental illness. The history of mental health care presented in many of these venues focuses on abuses in the past as well as on-going debates over the positive and negative aspects of diagnosis and various forms of treatment. In recent years the trend has accelerated, with several leading museums no longer defining themselves as repositories of the history of psychiatry but taking a wider approach to mental health as it is explored in science, society and culture. Broadening their interpretive framework beyond the practitioner perspective and the medical model, the Bethlem Museum in the UK was the first to rebrand as a ‘museum of the mind’ in 2015, joined soon after by the Dolhuys (‘crazy house’) in the Netherlands. From summer 2020, the Dolhuys and a related project, the Outsider Art Museum at the Hermitage in Amsterdam, will be known together as the Museum of the Mind (Museum van de Geest). In 2019, the Dr Guislain Museum in Ghent reopened with a redesigned permanent historical exhibition that shifts away from the iconic objects from the history of institutional care that were formerly on display, to draw more heavily on contemporary art addressing key themes, notably classification and power and powerlessness, alongside their extensive collection of art produced by people living in psychiatric facilities or with lived experience of mental illness (Allegaert et al, 2019).

‘Classification’ section of the new permanent exhibition at Dr Guislain Museum, Ghent, which opened in 2019. This artwork, ‘Fotonotities’ by Hans Eijkelboom, is displayed alongside historical photographs and artefacts
© Museum Dr GuislainExhibiting the history of psychiatry is of course complicated by the portrayal of mental illness and mental health care in popular culture and the news media, including terrifying depictions of punishment and restraint in dirty and dangerous asylums, and exaggerated portrayals of mental illness as a danger to society. While some of these representations are derived from a real and difficult history, such as the incarceration and mistreatment of vulnerable people, they also mythologise certain practices, especially the use of straitjackets or electro-convulsive therapy (known as ECT or ‘electroshock’).
Museums have an important role in challenging such misrepresentations, by explaining the therapeutic purpose behind them, as well as acknowledging the adapted but continuing use of restraint and ECT today. Yet as I have argued elsewhere, they have sometimes exaggerated the distinctions between historical and contemporary theories and practices to make a firm break with the past (Birdsall et al, 2015). Amidst concerns over ‘dark tourism’ (exploiting human suffering for entertainment), the potential of some exhibits to fuel negative stereotypes and stigma, and the risk of upsetting visitors with related personal experiences, some avoid discussion of the on-going use of techniques with negative associations, or relegate discomfiting objects to the outskirts of exhibitions or remove them to storage. Examples include the presentation of ECT as an outdated practice (as suggested in the former permanent exhibition of the Dolhuys Museum of the Mind in the Netherlands), and the removal of human remains from exhibitions and their deaccession at the Gothenburg Museum of Natural History (Högström and Gelang, 2020).
Like most medical museum collections, the historical artefacts and archives of psychiatric museums primarily represent the practitioner view, and so art has become an increasingly dominant strategy to incorporate the perspectives of mental health service users as well as to provide critical reflection on medical approaches, sometimes alongside oral histories or recordings of written accounts (which are harder to find). This has raised concerns among some curators and historians that the material culture of the history of psychiatry will be lost or endangered now it is fading out of favour for exhibition, and a push to acknowledge the research potential of such artefacts (Ankele and Majerus, 2020).
Where archival materials or historical objects are used, the juxtaposition of multiple perspectives from practitioners and service users can complicate simplistic negative assessments of historical approaches or contemporary treatments. A risk in this approach is that audiences struggle to synthesise competing views, so choose or remain on the side they are already most familiar with, rather than understanding the different dimensions that have shaped experiences of managing health and illness on both sides (Birdsall et al, 2015).
Perhaps most worryingly, as museums move away from chronologies of changes in medical theory and practice in favour of thematic exhibitions (such as those addressing labelling and treatment), the appeal to medical audiences – who could learn a great deal from these reinterpretations – may diminish. For example, a teacher who regularly takes nursing students to the Dr Guislain Museum reported that he finds the new exhibition harder to use for an historical overview than the previous version (personal communication with Verwegen, 2020). This is particularly unfortunate as health professionals who can appreciate the mistakes of the past, understand the shaping and reshaping of scientific knowledge and practice over time, and who can integrate the perspectives of those with lived experience into their approach, can improve medical research and healthcare. Other visitors have complained that the museum no longer matches their expectations, especially with the older version of the museum still depicted on numerous tourist websites and the iconic imagery of the history of psychiatry widespread in popular culture (interview with Lamot and de Voorde, 2020). Perhaps both of these issues will be solved as visitors get used to the new approach, but it is worth thinking about how the changing strategies of medical museums might be better adapted to suit different audiences.
Disability on display
https://dx.doi.org/10.15180/201406/003Similar challenges are relevant for the transformation of the representation of disability in medical museums, perhaps the most dramatic shift currently under way in the sector. While museums more broadly have focused primarily on access for disabled visitors and much less on their histories and culture, medical museums have commonly presented disability within exhibitions on the history of medical treatments and technologies, although most often in problematic ways. Objects such as an iron lung or an artificial limb are commonly shown alongside clinical images of children or adults with bodily differences caused by disease or genetics, replicating the medical gaze for the museum visitor.
Exhibitions have drawn on the medical model of disability, which prioritises ‘curing’ or ‘fixing’ differences, and ableist assumptions that life with a disability is a burden or a tragedy. Examples include displays of prosthetic limbs arranged to suggest a timeline of technical advances without attention to the experiences of wearers (who may have had more negative assessments of the limitations or discomfort of such items), or uncritical portrayals of medical ‘advances’ such as cochlear implants or genetic screening which do not address concerns that they are intended to eradicate deaf and disabled people. Such approaches fuel fear of disabled people and discrimination against them. Moreover, as disability theorists have demonstrated, ableism and the medical model influence the services healthcare professionals will recommend for disabled people and can directly endanger their lives (Longmore, 2003; Peña-Guzmán and Reynolds, 2019; Kukla, 2020). Instead, they propose the social model of disability, which as scholar Tom Shakespeare argues, acknowledges the lived realities of physical or cognitive impairment, but highlights how society’s attitudes, infrastructure and policies are far more disabling (Shakespeare, 2006).
Although reconsiderations of the representation of disability have occurred in several settings, the most consistent engagement is in the UK, in particular through the work of Leicester University’s Research Centre for Museums and Galleries. Looking at the accumulation of activities over the last fifteen years provides an interesting model for how such substantial shifts in interpretation could be productively handled. The Leicester group began surveying museum curators more broadly about the representation of disability in collections and exhibitions in 2004, concluding that only limited material was displayed and in ways that tended to confirm stereotypes. Museum holdings contained more relevant material than expected, but staff expressed concern about offending or distressing visitors and wanted guidance on appropriate ways to present these objects and histories (Dodd et al, 2004). The survey was followed by the project ‘Rethinking Disability Representation in Museums and Galleries’, which involved collaborative activities with nine museums of different types, including one medical collection at the Royal London Hospital Archives and Museum.[4] For this latter collaboration, a film-maker and archivist worked together to reinterpret the archive relating to Joseph Merrick, who had lived at the hospital, and who had become famous as ‘the Elephant Man’ through the writings and engravings of his physician, Sir Frederick Treves. The research inspired a series of questions posed to disabled people for a film in which they reflected on how they had learnt about the story of Merrick and the connections between his experiences and their own lives.
The team moved on to medical museums specifically with Stories of a Different Kind, which ran from 2012 to 2014, in which disabled artists developed performances reconsidering collections and histories traditionally presented in these spaces. The artist Mat Fraser created a live performance titled Cabinet of Curiosities: How Disability was Kept in a Box, which directly challenged the conventions of medical museum displays that present bodies and body parts as ‘specimens’ or medical cases illustrating particular disorders, without referring to the person they are from. He did so by reflecting on the history of the materials displayed and their relationship to contemporary attitudes towards disability. The website description of the projects stated their aim, to develop:
new ways of presenting disability in medical museums, as they hold some of the most significant collections relating to physical and mental differences but, in the past, have sometimes displayed them in ways that sit uncomfortably with contemporary, rights-based understandings of disability.
(University of Leicester, 2014), emphasis mine
This quotation exemplifies the tensions inherent in such work, most obviously the difficulty of pressing for changes in medical museums which call into question the beliefs and practices of the medical profession. Medical museums vary in the degree of critical commentary they include on discredited or contentious practices and ideas, but more generally celebrate medical accomplishments and honour major figures in history. Those still affiliated with medical schools or societies are especially closely aligned with the profession, and may include stakeholders as staff, in management or on an advisory board. The social model of disability incorporates a fundamental criticism of the role of medicine in creating cognitive and bodily ‘norms’ and imposing these through medical interventions to ‘correct’, ‘treat’, or ‘cure’. Although disability scholars have used the notion of ‘impairment’ to acknowledge the lived experiences of pain, distress or ill-health that medicine can be useful to address, they have also challenged overreach and the tendency in healthcare to locate disability solely in individual minds and bodies rather than recognising the role of social structures and standards in limiting quality of life. By locating the problem in the past (as museums of the history of psychiatry also often do), this quotation implies that attitudes have since changed and that it is only that medical museums need to catch up, without raising the more difficult issue of healthcare’s on-going commitment to the flawed and limiting medical model.
The Leicester team led a second, larger collaborative project on these themes from 2015 to 2017, ‘Exceptional & Extraordinary’, which brought artists and performers together with eight medical museums for a series of activities.[5] At the event I attended at the Hunterian Museum (located at the Royal College of Surgeons of England), Deaf Men Dancing gave a performance about the history of medical treatment and education for the deaf, emphasising its oppressive emphasis on speech and the suppression of sign language. Francesca Martinez performed a comedy routine, the ‘Wobbly Manifesto’, which focused on the value of a life with cerebral palsy, confronted ableist assumptions that such an experience would be tragic or a burden, and demonstrated how government policies limit the lives of disabled people, often in life-threatening ways. Both performances challenged the medical preference for ‘curing’ difference even at the expense of the quality of life of an individual, and presented stark criticisms of the mistreatment of deaf and disabled people as an on-going problem in medicine today (I, Science, 2016).
This critique of the continuing impact of such narrow medical perspectives was delivered to an audience including medical practitioners yet seemed so at odds with how the history of medicine was displayed in the museum where the event took place that it was difficult to imagine how the two perspectives might ever be reconciled. In the discussion session that followed the performance, comments were largely celebratory and safe, avoiding the question of whether a medical museum (especially one with a board of advisors from the profession and a large proportion of visitors also working in medicine) was willing to incorporate these critiques, or how they could do so.
At the time, I wondered if these artistic engagements might only offer temporary moments of reflection rather than spur more serious reconsideration of the strategies of permanent exhibitions. However, change has been slowly but surely underway, in the UK (and the participating museums), as well as more broadly. A growing number of museums have begun to collaborate more frequently with disabled people and to integrate their experiences into their interpretive frameworks. Recent examples include the National Museum of Scotland, Pauls Stradiņš Museum of the History of Medicine, Latvia, and the Museum of the History of Medicine of Catalonia, Spain.[6] The experiences of disabled people are integrated into the new Wellcome: The Medicine Galleries at the Science Museum in London and the social model was used to inform both the design and the content of the permanent exhibition gallery on contemporary medicine at Wellcome Collection, Being Human, which opened in 2019 (and which the Leicester University group advised on). The Accentuate Programme at Screen South has recently launched ‘Curating for Change’, working with twenty museums, including the Thackray Museum of Medicine in Leeds, to develop a model of co-production with disabled people. The project will also include a work placement programme for D/deaf, disabled and neurodiverse curators to address their under-representation across the cultural sector, as this is a major contributing factor to the under-representation of disabled people in exhibitions. Esther Fox, head of Accentuate, notes that medical museums have an opportunity to take the lead and inspire a wider shift, saying:
Disabled people are rarely represented in our museums, but medical museums, due to the nature of their collections, have more opportunities than most to grapple with the challenges of presenting nuanced and authentic experiences of disability if they are prepared to work with disabled people themselves to interpret their collections [emphasis in original].
Some of these museums now pay more attention than ever before to medicine’s role in defining ‘norms’ and declaring some people, characteristics or behaviours ‘abnormal’ or deficient, although as Fox concludes, ‘there is still more work to do to foreground lived experience as a validated form of knowledge alongside medical understandings’ (personal communication, 2020).
Colonial collections and contemporary legacies
https://dx.doi.org/10.15180/201406/004In the next few years, the colonial origins of medical heritage collections, the role of medical research in justifying racial inequality and discrimination, and the recent revival of racial science, will also receive increasing attention, from outside the museum as well as within. While contemporary research undermines the idea of genetically distinct races, museums were integral to the colonial project of collecting and codifying cultures and peoples in hierarchies organised in comparison to an idealised white race (Bennett, 2004). This function is especially significant in medical museums given the history of racial science, which was used to argue for biologically-based racial inferiority or superiority, and to justify unequal treatment (Redman, 2016). Race continues to be used as a category of differentiation, including within medical research and treatment, while racism endangers the health and wellbeing of people of colour in a complex constellation of ways, from increased exposure to health risks and restricted access to treatment, to discrimination by healthcare professionals (Saini, 2019; Gilman, 2013; Hoberman, 2012; Davis, 2019).
The role of ethnographic museums in particular in perpetuating racism and inequality, firstly, by withholding objects stolen or coercively removed from colonised peoples, and secondly, by displaying them in ways that confirm stereotypes and contravene the original owners’ cultural norms, is now widely acknowledged and leading to slow but deliberate change (Simpson, 1997; von Oswald and Tinius, 2020). An added incentive to embrace this work comes from the resurgence of racial science in recent years as well as emboldening of white supremacists. Indeed, history and medicine are frequently mobilised today to justify racism, placing medical museums well within such controversies whether they choose to explicitly enter the fray or not. As I wrote this article, the lack of attention to the history of slavery and the legacies of colonialism had become front-page news in the aftermath of the killing of George Floyd, as Black Lives Matter protests against racism and police brutality turned attention to monuments and museums that minimise or ignore this history in the USA, Belgium, the Netherlands, France and the UK (Siddique et al, 2020; The New York Times, 2020). In addition, the under-representation of Black, Asian and minority ethnicity staff at all levels in the museum profession, but especially in governance, is increasingly highlighted as an example of the broad gap between museum policies of inclusion and actual practice.
The reconsideration of the ownership and display of ethnographic collections already underway in some western museums has led to the repatriation of objects, the removal of sacred materials from display, and policies to enable communities to use museum collections for traditional practices, as well as efforts to recast racist exhibition narratives and end dehumanising displays (Crenn, 2017; Pagani, 2017). Although these activities are on-going and incomplete, the pace of change has quickened in recent years, most recently with a network of museums across Europe redefining themselves as ‘Museums of World Cultures’ committed to exploring the colonial history of their own institutions and collections (Levitt, 2015).
Medical museums have also reconsidered some aspects of collections and displays, particularly with regard to human remains, and objects have been repatriated or removed from display (Museum of New Zealand Te Papa Tongawera, 2019). However, a more explicit presentation of medicine’s colonial and racist histories has been slower to emerge. In fact, the presentation of race in these institutions has primarily remained limited to one familiar story, the rise and fall of eugenics. Museums follow the wider cultural narrative of the history of eugenics in which the field is often presented as a pseudoscience rather than a popular branch of respectable medicine, in a narrative arc that usually ends with an assertion that the extremes of the Nazi era tarnished the field and put an end to it (Birdsall et al, 2013).
In recent years a few major medical museums have taken on the subject in a more expansive manner. The Dresden Hygiene Museum presented ‘Racism: The Invention of Human Races’ from May 2018 to January 2019 (Meier, 2020). This project was explicitly tied to the history of eugenics, as the museum had disseminated eugenic ideas as part of its public health education work in the era of National Socialism, and the links to present-day racism were also addressed (interview with Christoph Windgender, 2019). This exhibition was cited as one of the major influences on a subsequent project at the Teknisk Museum in Oslo, ‘FOLK – From racial types to DNA sequences’, held from March 2018 to December 2019, which examined the history of anthropology in Norway and inequality today (Teknisk Museum, 2020; interview with Phil Loring, 2019). Both exhibitions attracted national and international media interest, and although temporary, brought new collaborations and perspectives inside the museum which will be, or have already been, incorporated into the on-going work of each institution in the form of new interpretive approaches to artefacts and plans for public events and future projects.
A broader consideration of the presentation of colonial history and racial science is also underway in the Netherlands. In 2018, the Rijksmuseum Boerhaave reopened with a new set of galleries after a major renovation. The exhibitions make stunning use of the buildings’ historical architecture and display a wealth of historically significant and intriguing artefacts, integrated with creative digital interactives and a particularly dramatic immersive experience in a recreation of Leiden University’s sixteenth-century anatomical theatre. In May 2019, the European Museum Forum awarded the institution the European Museum of the Year award, ‘the most prestigious museum award in Europe…promoting innovative approaches in the museum sector’ (European Museum Forum, 2020). Four months after the award was announced, in September 2019, Dutch museums made international headlines when the Amsterdam Museum declared they would no longer use the term ‘Golden Age’ (Gouden Eeuw) in their historical exhibitions and activities (Amsterdam Museum, 2019). As the curator Tom van Der Molen explained in the Museum’s press release about the decision:
[t]he phrase ‘Golden Age’ occupies an important place in Western historiography – one that is strongly linked to national pride. However positive aspects associated with the term like prosperity, peace, luxury and innocence reflect only part of the historical reality of this period. The term glosses over the many negative aspects of the 17th century, such as poverty, war, forced labour and human trafficking.
The decision to make a change in this use of terminology followed years of critique of the failure of Dutch museums, schools and universities, politicians and broadcasters, and much of the populace, to acknowledge the role of the slave trade in this era of massive expansion of the country’s wealth and international influence. The ‘Golden Age’ was not so golden for those people enslaved for its creation, critics argue, and the story of success as commonly presented ignores the brutality and profiteering that was integral to this history and which continues to shape the Netherlands today (Small, 2012; Savenije et al, 2014; Wekker, 2016).
The Amsterdam Museum’s declaration generated heated debate (Het Parool, 2019; Redactie, 2019; Boffey, 2019; Siegal, 2019). The controversy also presented difficulties for the Rijksmuseum Boerhaave, as a significant portion of their new permanent exhibition is titled, and devoted to, the ‘Gouden Eeuw’.

The Golden Age gallery at the Rijksmuseum Boerhaave, opened after an extensive renovation of the museum in 2017
© Rijksmuseum BoerhaaveWithin this gallery, there is no reference to the role of slavery in the creation of Dutch wealth and power, and explicit attention to the role of colonial activities (and colonised people) in the production of scientific knowledge is limited to one label. This mentions that German naturalist Maria Sibylla Merian travelled with her daughter to Suriname in the seventeenth century (when it was a Dutch colony) where, in collaboration with indigenous people, she documented the metamorphosis of insects. One of the highly celebrated digital interactives in this section, a process of dissection that a visitor watches projected on their own arm as if the layers of their own body were being peeled back, does not work on black skin, a problem that was not discovered until after the renovated museum reopened.[7]

Digital interactive which does not work on black skin, installed in the permanent exhibition of the renovated museum
© Rijksmuseum BoerhaaveA legacy project of the previous director, the exhibition represents a traditional approach to Dutch history which remains fairly prevalent in textbook and public histories, although in the last few years several high-profile projects have begun to shift the narrative, including maps, guides and tours of slavery heritage, the founding of the Black Archives, memorial events commemorating the end of slavery in Dutch colonies, and museum exhibitions ( Hondius et al, 2014). The arrival of Amito Haarhuis as the Museum’s new director in April 2018 has also ushered in a new phase at the Boerhaave. As he recounts:
When I first visited the museum with my black husband, I felt shame when looking at the showcase with Petrus Camper’s engravings without a present day context (see Figure 6). My main problem with the old text was that Camper’s work was explained in the context of his time, praising him for going against the present opinion at the time. But the text didn’t say anything about the fact that Camper’s system was misused by others to justify slavery and racism…and that according to present day biology there is no such thing as different races within the species Homo sapiens.

Section of the permanent exhibition where label text accompanying the engravings by Petrus Camper was rewritten to address the misuse of his work to justify slavery and racism
© Rijksmuseum BoerhaaveAlthough he would not usually interfere directly with exhibition texts, Haarhuis asked staff to revise the interpretation in this section to address these missing issues, and two labels were rewritten (including a second on the German physician and founder of phrenology, Franz Joseph Gall). Other initiatives followed, including a wider reconsideration of all the museum labels, in which staff applied the recommendations of a recent guide to inclusive museum language, and the organisation of an international workshop on race and collections suggested by one of the curators, Bart Grob. We organised this event together, and ‘Race in the Medical Museum: Collections and Exhibitions’ was held at the Boerhaave on 22 November 2019. The lack of diversity among medical museum staff was evident as the invitee list was compiled, and the planned date was postponed once to allow for a wider range of participants. Attendees included primarily curators and other museum staff, alongside some academic researchers working on museum issues. Most gave short presentations about objects related to ideas about race from (their) particular museum collections. Our discussions explored materials labelled problematic or useful for exhibiting ideas about race, as well as the various actions taken with such materials and the potential for engaging audiences in the future.
Three conclusions from these conversations are particularly useful for the discussion here. A starting point, raised by attendee Shelley Saggar, a research fellow at the Science Museum in London working on culturally sensitive objects, would be to recognise that ‘difficult’ histories (as race and racism might be labelled by White museum stakeholders) are essential subjects for Black, Asian and minority ethnic museum staff and visitors. While White staff might think it is risky, upsetting or uncomfortable (for everyone) to exhibit these painful pasts, Black, Asian and minority ethnicity groups are already discussing these histories, and in fact cannot avoid them as they encounter the negative consequences today.
A second conclusion is the importance of not restricting this history to limited interventions or temporary exhibitions but instead to more drastically revise the narratives presented in museums to acknowledge a shared past. The goal is not to simply acknowledge slavery underpinning trade and wealth, or to mention the role of colonised researchers in the development of western science, for example, but to acknowledge the always inter-related lives of our intertwined past and to explain what is at stake in the way we have told these histories. Common objections I have heard from museum staff regarding each of these ideas include a lack of space and a lack of audience interest in such meta-level reflection. As I discuss in my conclusion, instead of cabinets of curiosities, the display of fewer items would allow for deeper engagement with their meanings, and resources devoted to in-gallery activities would enable a wider array of engagement (rather than simply the addition of more text, or more objects, as opponents seem to assume). Exploring with visitors why certain narratives are privileged, and what the consequences are of framing histories in certain ways, is surely a more effective way to question and reshape cherished or previously unquestioned narratives than by simply asserting the past they have learnt is wrong.
Although our host at Boerhaave was interested in the development of guidelines for best practices regarding what can or cannot be shown, and what should or should not be said about it, it became clear during the workshop that it would be difficult to find any such consensus within such a small group, let alone across audiences. This informed the final conclusion I include here, that museums need to give up some authority and raise questions but not always answer them. Such an approach is sometimes used by institutions as a way to avoid taking a side in a contentious issue, and may leave some visitors unsatisfied or confused due to competing or unclear messages. Yet in the context of shifting discussions, finding ways to create more room for debate within exhibition spaces seems preferable to trying to freeze definitive statements in time in exhibition interpretation.
Reproducing bodies
https://dx.doi.org/10.15180/201406/005A final area of work where I see great potential for medical museums to innovate is regarding representations of reproduction. The history of sexology is a popular exhibition theme but not infertility, pregnancy, pregnancy loss, abortion or childbirth, and while these are admittedly less ‘fun’ topics than the history of research on sexual behaviour they are no less relevant. This paradox is also evident in wider society, where the sexualised female body is everywhere to be seen, from advertisements to art galleries, yet her reproducing body is barely visible. We rarely see graphic depictions of childbirth, or realistic, non-romanticised representations of the physical changes involved in pregnancy and post-partum.
In medical museums, reproduction is represented predominantly by embryological models and the wet specimens of foetuses commonly referred to by curators as well as visitors as ‘babies in bottles’ (Parry, forthcoming 2021). Indeed, the most common materialisations of pregnancy in museums are human embryos and foetuses, with women literally cut out of the picture in anatomical models detailing reproduction and childbirth. These might be shown alongside practitioner tools, such as forceps, again with women notably absent.
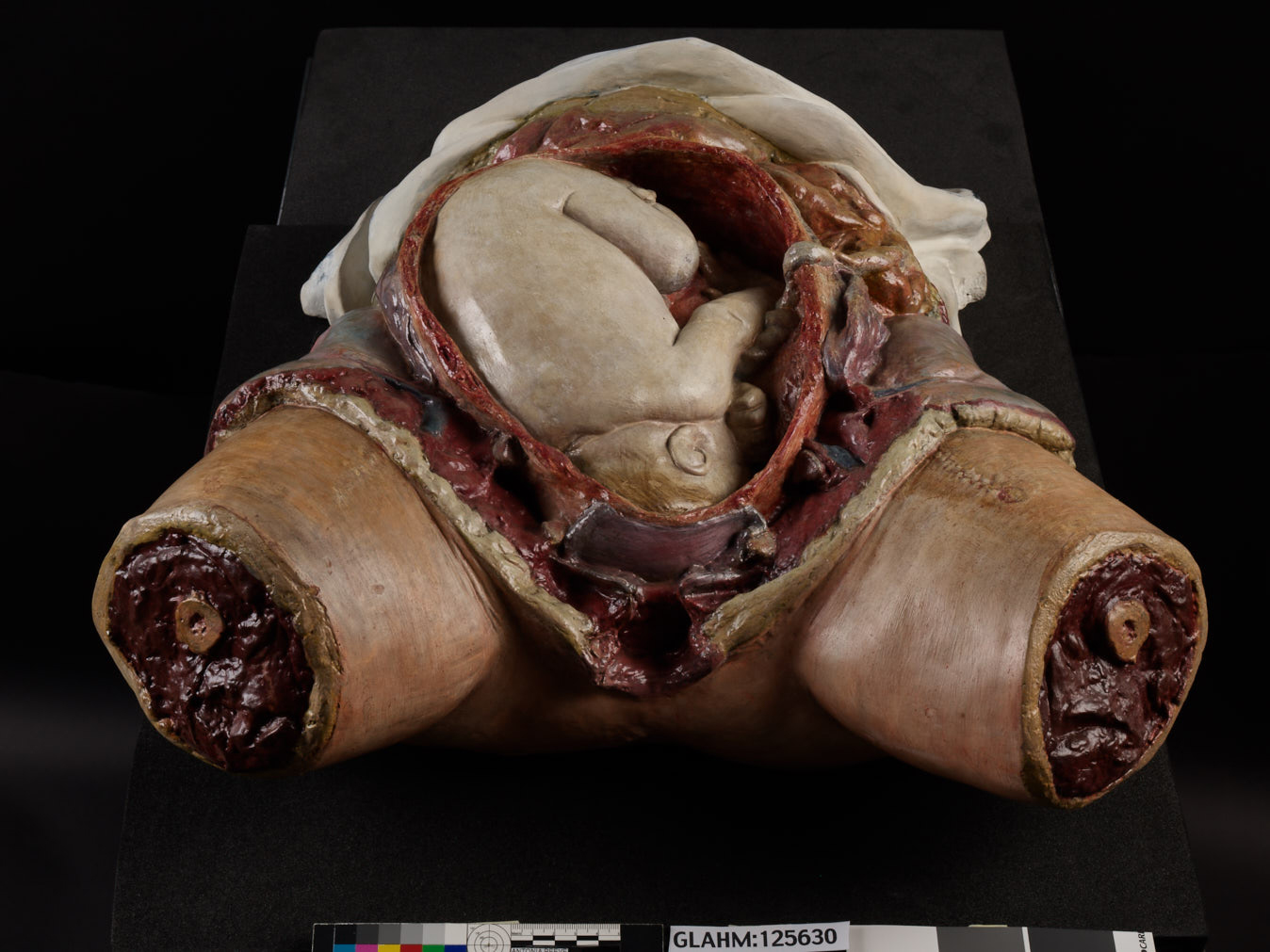
Plaster cast model of a foetus in the womb, based on dissections by Dr William Hunter, c 1750
© The Hunterian MuseumCurators and tour guides note that all of these objects can generate affecting responses from some visitors, especially women, who sometimes share their personal experiences with prenatal testing, having a miscarriage or difficult birth, or raising a disabled child (Tybjerg, 2019; Parry, 2020). All of these issues are considerations familiar to parents and people trying to conceive, yet they remain private topics, marginalised in culture and public debate. Given that around twenty per cent of known pregnancies end in pregnancy loss, the silence surrounding miscarriage is particularly problematic (Danielsson, 2020).
Women who have terminated a pregnancy or experienced a miscarriage due to the results of prenatal screening are also known to visit medical museums to learn more about a particular condition, or as part of their grieving process. At the Narrenturm in Vienna, for example, where there is an on-going collaboration with genetics researchers, one doctor even advises pregnant women to view the foetal specimens while they wait for their test results (interview with Edmund Winter, 2018). While such encounters offer a very limited, medical perspective, focused on the most extreme variations and the worst outcomes, they provide one of very few opportunities to see some of the developments in utero that may have played a role in a visitor’s own pregnancy and which inform the contemporary debate about reproductive choice and disability rights.
Curators debating whether to exhibit these collections acknowledge the difficulties they present. Firstly, there are the problems associated with the display of unusual anatomies or deformities, as discussed previously in relation to the representation of disabled people in medical museums. Some curators also expressed their concern that for adolescent girls especially, such exhibits may negatively affect their views on having children by creating an exaggerated sense of pregnancy risks (interview with Thomas Schnalke, 2019). This is of course exacerbated by the medicalised representation of pregnancy and childbirth in the mass media as well as widespread ableism, which undervalues and restricts the lives of disabled people.
Secondly, some visitors may interpret foetal specimens through the lens of contemporary abortion politics, but often without an understanding of the shifting landscape of health risks in the past or the current context of prenatal testing. The increasingly complex interaction between disability rights and reproductive choice in public debate, medical protocol and the law simplistically pits each against the other without acknowledging the shared challenge of inadequate social support for raising a disabled child and ongoing stigma and discrimination (Herzog, 2018). Medical museums could make a valuable contribution by including the lived experience of disabled people who have genetic conditions, as well as feminist perspectives on reproductive choice, and exploring the intersections between the two. As critical disability scholars discuss the ‘new eugenics’ of contemporary medicine and public health policy, especially genetic testing or the allocation of limited resources (as occurred during the peak of hospital admissions for COVID-19, for example), these collections also offer valuable opportunities to provoke visitor curiosity and engage with them about these issues (Darr, 2017; Brown et al, 2019). Yet even this very limited entry point is under threat as some museums remove these materials from display.
In my view, the important role that these displays play in generating conversations around reproduction, and prompting reflection, is underestimated by the stakeholders who argue against their exhibition. Instead, I advocate for the continued use of these collections, but crucially, that they need to be shown alongside a much wider representation of the realities of human reproduction than is commonly shown in medical museums. In fact, given the cultural silence on these issues, medical museums have a responsibility to address them. There is also a growing call for more attention to women’s reproductive health, to challenge stigma, abuse and commercial profit, all influenced by ignorance and shame surrounding the female body (Dusenbery, 2019; Gunter, 2019; Topping, 2020). The topic has been so overlooked that medical museums often have very limited materials however, as the Science Museum, London, recently realised when reviewing their expansive holdings of more than seven million objects. To address the under-representation of women’s reproductive health they initiated a new collecting project to gather artefacts and solicited suggestions from the public for possible items to include (Davies and Humphreys, 2019).
Alternative projects are also stepping in to fill the gap, such as the Museum of Contraception and Abortion in Vienna, founded by the gynaecologist Christian Fiala in 2007, and housed in the same building as his clinic (Museum of Contraception and Abortion, 2020). The Museum has a collection of around 3,000 objects sent from all over the world, as well as a library of scanned books that can be downloaded from their website. Despite repeated government interference and occasional protests, the Museum regularly attracts school groups as well as health professionals and general visitors, including international tourists (interview with Christian Fiala, 2018). Perhaps unsurprisingly given the medical background of the founder and location of the museum in the same building as his medical practice, the exhibition narrative contrasts the kitchen table of the illegal abortionist with the modern clinic situated across the hall, echoing the emphasis on medical progress that is common to the limited attention for this history in medical museums more broadly (although there is also attention to the social history of the struggle to control fertility and the political battles over legal abortion).
A similar impulse to address under-representation and to mobilise the cultural prestige and educational impact of museum exhibitions inspired Florence Schechter to open the Vagina Museum in London in 2019 (Vagina Museum, 2020). The aim of the project is to spread knowledge, erase stigma and raise people’s confidence to talk about anatomy and health, all aims that historical collections in medical museums are mobilised for in relation to other topics, and yet not for reproductive health (interview with Florence Schechter, 2020). While some might consider this example a public engagement activity rather than a museum in the usual sense, the goal in the future is to draw on existing museum collections as well as perhaps build some of their own. The press coverage that the Vagina Museum has generated indicates the potential popular appeal, and much of this coverage highlights the negative health impact of silence and shame around women’s sexual and reproductive lives (Marsh, 2019; Haynes, 2019; Wilson, 2020).
Finally, the Birth Rites Collection founded by the curator Helen Knowles and displayed at King’s College London, is intended to raise debate about the politics and practice of birth through exhibiting contemporary art on the topic (Birth Rites Collection, 2020).

'Home Birth (with vacuum cleaner)', C_Type Photograhic Print 9” x 12” by Eti Wade, 2001, one of the artworks that generated objections when displayed as part of the Birth Rites Collection
© Eti Wade and the Birth Rites CollectionThe project has encountered criticism from some of the obstetricians and gynaecologists on campus. One of the physicians argued against ‘the display of explicit artwork focusing on sexual and childbearing attributes of women in a learning and working environment’, and some of the works shown challenge the dominance of medicalised approaches to childbirth (interview with Hermione Wiltshire, 2020; Knowles and Wiltshire, 2019). Such objections, at a site where future midwives, gynaecologists and obstetricians are trained, indicate a damaging divide between practitioners and patients, and between medical ways of viewing the world and other forms of knowledge that are also valuable for managing health and healthcare.
Conclusion
https://dx.doi.org/10.15180/201406/006I have argued here that medical museums need to address risky issues, and present ‘difficult’ objects for public engagement, as a way to create complex stories, which acknowledge the mistakes of the past as well as their traces in the present. Setting aside histories that reflect poorly on the medical profession or which address topics that are currently controversial does little to rehabilitate the difficult aspects of the history of medicine, and medical museums, which continue to shape lived experience today. Instead, museums and curators need to experiment with exhibition strategies that encourage a more diverse audience, including those working in medical research or the provision of healthcare, to appreciate the development of ideas in their context and the factors that ensured the dominance of some views over other approaches; to connect the ideas and practices of the past with their contemporary legacies; and to navigate the competing theories and different communities of expertise that are relevant for managing health and wellbeing today.
In this brief conclusion I propose three strategies that I hope may be useful in this process. First, in contrast with the ‘cabinet of curiosities’ approach, I suggest museums show fewer things, and instead of spending resources on larger-scale exhibitions, invest more of the budget in on-going activities where visitors can interact with the items on display, with on-gallery staff, and with one another. This allows riskier histories or challenging objects to be shown, as it creates more space to explain the materials themselves and various interpretations, to discuss motivations for displaying them, and to respond to visitor reactions such as shock, ridicule, confusion, anger, sarcasm or joy. I see this as part of the traditional exhibition function of a museum, however, rather than separate special events, as the latter are more likely to be attended by a self-selecting audience, leaving objects from the permanent collection unseen or without context for those visitors who do not attend.
Second, museums could prioritise temporary exhibitions instead of permanent ones. Rather than investing resources in flagship projects that are intended to stay on display for many years, medical museums can better respond to breaking issues with shorter-term projects which also allow more risks to be taken. Curators can capitalise on controversies to show how collections connect to contemporary issues, and can also adapt projects, or revisit topics, as social mores regarding them change, if strong and valid criticisms are levelled at specific projects, or in light of new information or materials that could be incorporated into the histories displayed. Such an approach also allows the museum to keep up with the pace of change surrounding highly contested topics, meaning they do not have to avoid issues that are in flux in case their approach becomes rapidly out-dated, and can instead deliberately tackle issues with such high social relevance. An additional dimension for such work is to move outside the museum and collaborate with partners in other venues who are already engaging with diverse communities and using new approaches.
If temporary or external exhibitions are undertaken alongside more traditional permanent projects however, the insights and approaches generated in these need to be integrated into the permanent exhibition, and not just used as a release valve intended to subdue criticisms about this or the museum as an institution. Temporary exhibitions are often used in this strategic manner, leaving them on the margins of the main museum mission and meaning that the important work they have done to revise interpretation is lost when the short-term exhibition closes.
Third, the museum sector should support and reward new measures of impact and success, moving away from visitor numbers to evaluate the quality of interactions between visitors and on-gallery staff and the exhibitions and activities, the range of partners involved, and the diversity of strategies used. It is particularly important that expectations of celebratory press coverage or assumptions of visitor disinterest in difficult topics are challenged. The media often ignores ‘marginal’ groups and projects about them, and rewards familiar approaches while amplifying controversy over unusual ones. All of this discourages museum leaders from tackling important topics and reaching out to certain potential audiences.
Moreover, even in medical museums, decision-makers often doubt the appeal of subjects assumed to be sad, or to underestimate their relevance for a broad audience. This often reflects misunderstandings, such as assumptions that people do not want to reflect on death and pregnancy loss in a museum setting, or that mental health issues or disability are of interest only to a minority, rather than relevant to everyone. However, projects that have a direct relevance for a small group should not be ignored in favour of only issues assumed to have mass appeal. The two strategies above would allow museums to experiment with topics otherwise considered niche or distinct target groups, to serve discrete audiences, and perhaps also expand notions of who is interested in what. Finally, evaluations of all of these activities need to be made widely available so that museums can work with evidence instead of assumptions and learn from the activities of one another. In these ways, medical museums can embrace the risks of exhibiting some of the difficult histories preserved in their collections and the objects that so powerfully invoke them.
Tags
Footnotes
References
Media in article







